







Bone Remodeling in the Alveolar Ridge

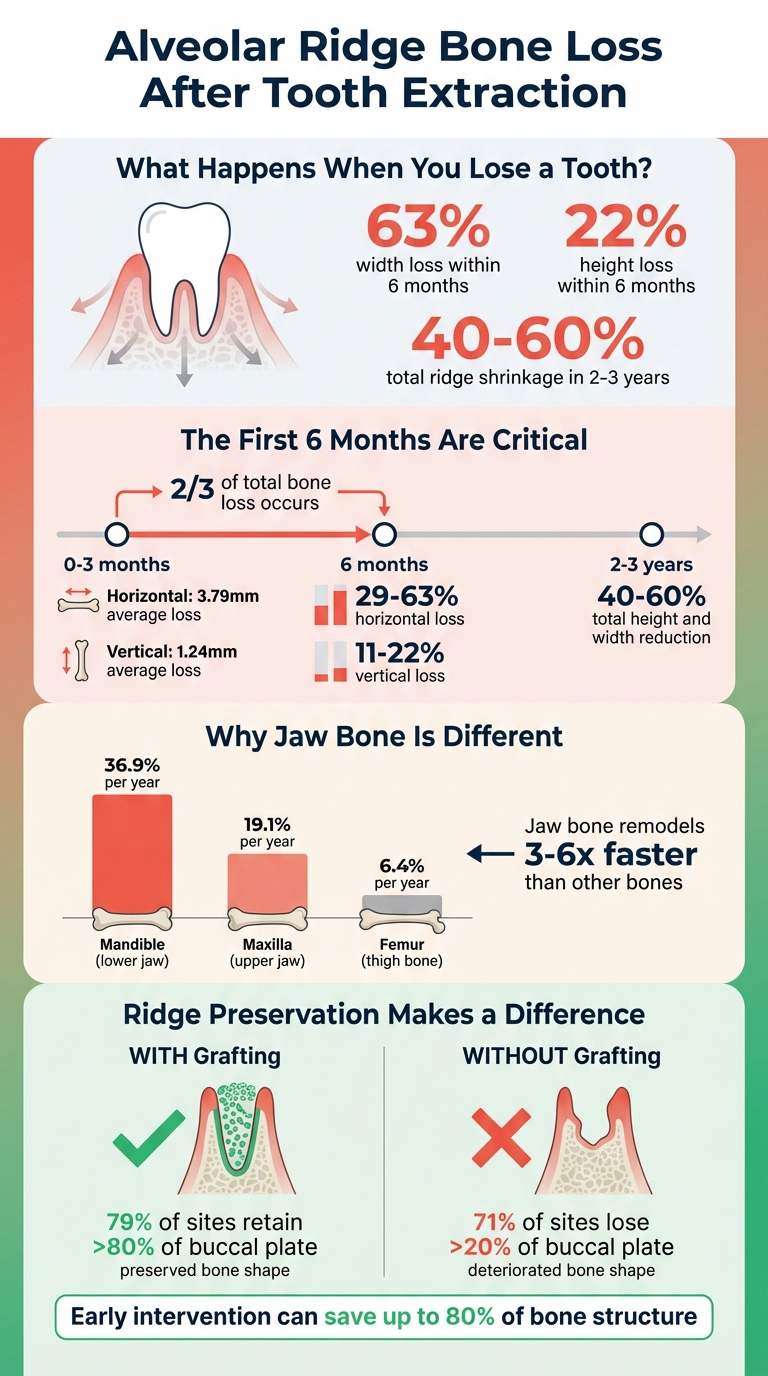
Losing a tooth doesn’t just affect your smile – it triggers a rapid transformation in the alveolar ridge, the bone that holds your teeth in place. Within six months of tooth loss, up to 63% of the ridge’s width and 22% of its height can disappear. This dramatic change impacts dental implants, dentures, and even facial structure. Why does this happen? The alveolar ridge relies on chewing forces to maintain its shape. When those forces stop, the bone begins to shrink.
Here’s the process in a nutshell:
- Bone Remodelling: The ridge has an unusually high turnover rate – up to 36.9% yearly in the lower jaw.
- Tooth Loss Impact: Without a tooth, the ridge quickly shrinks, especially the buccal plate (outer bone wall).
- Healing Phases: After extraction, the socket heals in three stages – clean-up (inflammatory phase), new bone growth (proliferative phase), and refinement (remodelling phase).
- Preservation Options: Techniques like atraumatic extractions, bone grafts, and barrier membranes can reduce bone loss and prepare for future implants.
To avoid complications, early intervention is key. Ridge preservation during tooth extraction can save up to 80% of the bone structure, making future dental work easier and more reliable.
Alveolar Ridge Bone Loss After Tooth Extraction: Timeline and Statistics
Alveolar Bone Remodeling: Mechanisms, Significance, and Regenerative Advances in Dentistry
sbb-itb-2be92ed
The 3 Phases of Bone Remodelling
After a tooth extraction, the alveolar socket undergoes healing in three overlapping phases, each marked by distinct cellular activity and structural changes. These phases highlight why the ridge changes so noticeably after tooth loss and why precise timing is crucial for general dental treatments that follow.
Inflammatory Phase
Right after the tooth is removed, a blood clot forms in the socket. This clot, rich in fibrin, provides a stabilised framework for the repair process to begin [8]. Within the first 24 hours, neutrophils and macrophages move into the clot and surrounding connective tissue [8][2]. These cells clear away debris and release chemical signals that attract the next wave of cells needed for regeneration. At the same time, granulation tissue starts to form, preparing the area for new tissue growth. Once the inflammatory cells have done their job of cleaning up and initiating signals, the process transitions to active tissue regeneration.
Proliferative Phase
By the third day, fibroblasts begin infiltrating the clot, and osteoprogenitor cells expressing Runx2 appear along the socket margins [4][2]. This marks the start of tissue regeneration. The blood clot is gradually replaced by granulation tissue [4][9]. Osteoblasts then step in to deposit osteoid, leading to the formation of new bone. By around eight weeks, trabeculae of bone occupy most of the socket [4]. Woven bone typically starts forming at the apical and lateral walls, gradually extending toward the centre [4]. In humans, the apical two-thirds of extraction sockets are often filled with soft, cancellous bone by 10 weeks, and the entire socket is generally filled by 15 weeks [4].
"The elevation of a flap might diminish the ability of periosteal cells to regenerate bone, while an undisturbed periosteum maintains its osteogenic potential." – Giorgio Pagni et al. [4]
Bone Modelling and Remodelling Phases
Once the initial bone has been deposited, the process shifts to refining and maturing the alveolar ridge. Immature woven bone is gradually replaced with mature lamellar bone [10][11]. At the same time, the alveolar ridge undergoes modelling – a process that changes its size and shape in response to mechanical forces [10][11]. Bone modelling involves resorption and formation occurring on different surfaces, while remodelling is a renewal process where resorption and formation happen sequentially at the same site [11].
The bundle bone, which previously anchored the tooth’s periodontal fibres, is among the first to be resorbed since it no longer serves a purpose after tooth loss [4][2]. This explains why horizontal ridge shrinkage (29–63%) is typically more pronounced than vertical bone loss (11–22%) within six months of extraction [4]. The ridge continues to shrink until mechanical strain stabilises, aligning with Wolff’s Law [7][3].
| Feature | Bone Modelling | Bone Remodelling |
|---|---|---|
| Role | Alters size and shape; adapts to mechanical loads [10][11] | Renews skeleton; repairs microdamage [10][9] |
| Coupling | Resorption and formation occur on different surfaces [11] | Resorption and formation happen sequentially at the same site [11] |
| Alveolar Effect | Leads to ridge contraction after tooth loss [7][4] | Replaces woven bone with mature lamellar bone [7][4] |
Cellular and Molecular Mechanisms
The continuous cycle of bone breakdown and renewal in the alveolar ridge is driven by three specialised cell types. First, osteoclasts – large, multinucleated cells – dissolve both the mineral and organic components of bone. They form a sealed zone on the bone surface and release hydrogen ions and enzymes like cathepsin K to break down the matrix.
Once resorption is complete, osteoblasts take over to build new bone. These cells not only construct bone but also regulate its turnover by secreting factors like RANKL, which promotes resorption, and osteoprotegerin (OPG), which inhibits it. The interplay between RANKL and OPG is crucial in maintaining bone balance.
Osteocytes, making up 90–95% of all bone cells, are former osteoblasts embedded within the mineralised bone. Acting as mechanosensors, they detect strain from activities like chewing and identify microdamage. These physical signals are then converted into biochemical cues, triggering bone remodelling.
"The RANKL/OPG expression ratio determines the degree of osteoclast differentiation and function." – Liza J Raggatt, Faculty of Health Sciences, The University of Queensland [12]
The balance of bone turnover is further influenced by hormones and signalling molecules. For instance, parathyroid hormone (PTH) binds to osteoblast receptors, boosting RANKL production and recruiting osteoclast precursors to promote resorption. PTH also inhibits sclerostin, a protein from osteocytes that suppresses bone formation via the Wnt signalling pathway. On the other hand, calcitonin directly targets mature osteoclasts, reducing their activity and slowing down resorption.
The shift from bone breakdown to formation depends on coupling signals. As osteoclasts resorb bone, they release growth factors like transforming growth factor beta (TGF-β) and insulin-like growth factor 1 (IGF-1) from the bone matrix. These factors attract osteoblasts to the site. Additionally, communication through EphB4–ephrin-B2 interactions helps balance resorption and formation. This dynamic process contributes to the alveolar ridge’s high turnover rate – 19.1% in the maxilla and 36.9% in the mandible – compared to the slower turnover seen in long bones [13][2].
Clinical Effects of Alveolar Bone Loss
Dimensional Changes in the Alveolar Ridge
When a tooth is removed, the alveolar ridge begins to undergo significant and irreversible resorption almost immediately [15][16]. This process starts with the rapid resorption of bundle bone and subsequent remodeling of the outer bone surface, leading to both horizontal and vertical shrinkage of the ridge [4][14].
The buccal plate, which is particularly thin – about 0.8 mm in the anterior region and 1.1 mm in premolar areas – is especially vulnerable to this resorption following extraction [4][14].
Within just six months, the ridge can lose approximately 40% of its height and 60% of its width [16]. Most of these changes occur early on, with two-thirds of the total hard and soft tissue loss happening in the first three months [4]. By six months, horizontal bone loss typically ranges from 29% to 63% (an average of 3.79 mm), while vertical loss on the buccal side is between 11% and 22% (an average of 1.24 mm) [4].
"The height of a healed socket never reaches the coronal level of bone attached to the extracted tooth." – Giorgio Pagni et al., University of Milan [4]
Long-term studies reveal that within the first two to three years, the alveolar ridge can shrink by 40% to 60% in both height and width [4]. For some patients, this bone resorption continues throughout their lifetime, leading to cumulative losses that can significantly impact their quality of life [6]. The mandible tends to experience more height loss, while horizontal resorption is generally more pronounced in the maxilla [14].
These changes not only affect the structural integrity of the ridge but also have a direct impact on the overlying soft tissues and the success of future restorations.
Effects on Soft Tissue and Restorations
The resorption of the alveolar ridge alters the bony framework, which in turn destabilises the soft tissues and compromises dental restorations. As the bone diminishes, the facial gingival contour collapses, and the height of the interproximal papilla decreases – an issue that is especially noticeable in the aesthetic zone [16].
These bony changes lead to ridge deformities, complicating the design of bridge pontics and reducing the retention of removable dentures [16]. Prolonged use of dentures can further accelerate ridge resorption [6]. Additionally, soft tissue width at extraction sites may decrease by an average of 6.1 mm over a 12-month period [6].
Reduced bone volume also makes dental implant placement more difficult. Horizontal bone loss can leave the ridge too narrow for standard-diameter implants, while vertical loss may result in overly long clinical crowns or exposed implant threads, affecting both implant stability and hygiene [4][14]. A sloped ridge, caused by greater vertical loss on the buccal side compared to the lingual side, adds further challenges to achieving optimal implant positioning and aesthetics [1].
"The survival of implants and their ability to provide adequate function and esthetic are strictly correlated with their proper positioning in relation to the alveolar housing, the neighbouring teeth and the occluding dentition." – Giorgio Pagni et al. [8]
Without preventive measures at the time of tooth extraction, the extent of bone loss can make ideal implant placement extremely difficult, often requiring secondary procedures to augment the ridge [14][16]. Even the most skilled surgeons cannot reliably predict how the buccal plate will behave over time, highlighting the importance of considering ridge preservation techniques during the extraction process [4].
Alveolar Ridge Preservation Methods
The future of the buccal plate after tooth extraction can be uncertain, so it’s often better for clinicians to focus on ridge preservation techniques during extraction rather than waiting to tackle bone loss later. These methods aim to reduce dimensional changes and keep enough bone volume to support implants or prosthetic work down the line.
Atraumatic Extraction Techniques
How a tooth is removed plays a big role in preserving bone. Flapless extraction is a key method because it helps maintain the periosteal blood supply and the osteogenic cell layer, both of which are crucial for bone regeneration [4].
For multi-rooted or single-rooted teeth, sectioning the tooth can minimise the force needed for extraction, which protects the delicate alveolar walls [18]. Tools like periotomes or luxators are designed to sever periodontal fibres gently, avoiding the heavy-handed use of forceps that might damage the thin buccal plate [4][18].
Another approach is the socket-shield technique, where part of the buccal root is left in place. This helps preserve the periodontal ligament and bundle bone, reducing the risk of buccal ridge collapse [18].
After extraction, choosing the right biomaterials for periodontal regeneration becomes essential to reinforce these preservation efforts.
Bone Graft Materials and Membranes
Bone graft materials act as scaffolds, helping to maintain bone volume for future restorative work [4]. Here’s a breakdown of the main types:
- Autografts: Taken from the patient’s own body, such as the maxillary tuberosity or chin, these grafts are considered the gold standard. They offer properties that promote bone growth (osteogenic), stimulate new bone formation (osteoinductive), and provide a structure for bone to grow on (osteoconductive).
- Allografts: Sourced from human donors, these include Freeze-Dried Bone Allograft (FDBA), which is primarily osteoconductive, and Demineralised Freeze-Dried Bone Allograft (DFDBA), which is both osteoconductive and osteoinductive due to exposed bone morphogenetic proteins (BMPs). Studies show that DFDBA results in a higher percentage of vital bone – 38.42% versus FDBA’s 24.63% – within four to five months [19].
- Xenografts: Usually derived from bovine sources, these are osteoconductive and break down slowly, making them ideal for long-term space maintenance.
- Alloplasts: These synthetic options, like hydroxyapatite (HA), tricalcium phosphate (TCP), and bioactive glass, are osteoconductive and carry no risk of disease transmission. Bioactive glass, in particular, has shown impressive results, with up to 59.5% vital bone formation at six to eight months post-extraction [19].
Barrier membranes are another critical tool in ridge preservation. These are used in Guided Bone Regeneration (GBR) to stop soft tissue from invading the extraction site, giving osteoblasts – the cells responsible for bone formation – time to do their work. Resorbable membranes, such as those made from collagen, naturally dissolve and eliminate the need for a second surgery. Non-resorbable membranes, like ePTFE or titanium, provide better space maintenance but require surgical removal [4][17]. Research suggests that using a non-resorbable membrane without primary wound closure may promote more effective new bone formation compared to forced primary closure [17].
Clinical findings highlight the benefits of grafting: 79% of grafted sites experienced less than 20% buccal plate loss, while 71% of non-grafted sites lost more than 20% of the buccal plate [4]. By grafting during extraction, the need for additional surgery to prepare the implant site is often avoided [20][4].
These techniques not only limit further bone loss but also lay the groundwork for successful restorative procedures, working in harmony with the natural bone remodelling process discussed earlier.
Factors That Affect Bone Remodelling
Building on the understanding of cellular mechanisms, it’s essential to consider the external influences on bone remodelling in the alveolar ridge. Both systemic and local factors play a crucial role in determining how effectively bone regenerates after tooth loss. These insights help clinicians predict challenges and customise treatment strategies.
Systemic Factors
Hormonal changes significantly impact bone remodelling. For instance, oestrogen deficiency – common during menopause – speeds up bone loss by increasing RANKL activity while reducing osteoprotegerin (OPG), leading to greater bone resorption [21]. Women may experience up to a 9% reduction in bone mass during lactation due to parathyroid hormone-related peptide (PTHrP) [22]. On the other hand, testosterone promotes bone and muscle growth, and its decline in older men is a known contributor to osteoporosis [21].
Parathyroid hormone (PTH) also plays a systemic role, responding to low calcium levels by modulating RANKL activity [3]. Chronic stress or glucocorticoid treatments elevate cortisol, which reduces bone formation by prolonging osteoclast survival and inducing osteoblast apoptosis [3, 29]. Conditions like diabetes mellitus further complicate bone formation through prolonged inflammation and delayed gingival healing [21]. Additionally, vitamin D deficiency can lead to secondary hyperparathyroidism, which increases bone resorption [3].
Interestingly, the alveolar bone remodels much faster than other skeletal sites. For example, the mandible has a turnover rate of about 36.9% per year, compared to only 6.4% in the femur [2]. With the global ageing population expected to reach 1.5 billion by 2050, the prevalence of periodontitis among adults aged 65 and older is projected to rise by 50% by 2040 [21].
Local factors also play a key role in shaping the mechanical environment of the alveolar ridge, directly influencing bone remodelling outcomes.
Local Factors
While systemic signals regulate cellular activity, local forces and conditions have an equally critical impact. Mechanical loading is one of the most direct influences. According to the mechanostat theory, bone mass decreases when strain falls below a certain threshold – such as when a soft diet reduces chewing forces – and increases when strain exceeds functional levels [2]. As Maiko Omi from the University of Michigan explains, "Bone is more sensitive to dynamic strain changes rather than static strain" [2]. Bone remodelling typically occurs within a strain range of 2,500–4,000 microstrains, while exceeding 4,000 microstrains can lead to pathological resorption [24].
Chronic infections like periodontitis also disrupt bone metabolism. Bacterial components, such as lipopolysaccharides, activate the RANKL/OPG system, encouraging excessive osteoclastic activity and suppressing osteoblast differentiation [2, 34]. This creates a hypoxic and acidic microenvironment, further increasing bone resorption while hindering new bone formation [9].
Physical trauma introduces another layer of complexity. Microcracks in the bone matrix can result from trauma, and the death of osteocytes in these areas removes inhibitory signals, prompting targeted remodelling to repair the damage. Resorption sites are three times more likely to form near microcracks [9]. Additionally, factors like the number of remaining bony walls and defect size directly affect blood supply and the availability of osteogenic cells [23]. Clinical research on guided bone regeneration shows that sites without membrane exposure can gain 1.1 to 3.1 mm more new bone compared to those with exposure [25].
Conclusion
Alveolar bone remodelling plays a crucial role in shaping treatment plans. Studies highlight that about 50% of the crestal width is lost within 12 months after tooth extraction, with average reductions of 3.79 mm horizontally and 1.24 mm vertically within the first six months. These changes significantly affect implant positioning and their long-term success [4].
The underlying cause of these changes lies in the alveolar bone’s unique cellular activity. Its turnover rate is three to six times higher than that of the femur [2]. When a tooth is removed, the lack of functional strain leads to disuse atrophy, which accelerates bone loss.
This understanding has direct clinical implications. Research indicates that 79% of grafted sites retained over 80% of the buccal plate, while 71% of non-grafted sites experienced more than 20% loss [4]. Early interventions, such as socket grafting, atraumatic extraction techniques, and careful biomaterial selection, can significantly reduce the need for invasive procedures later on. For implants, which require a minimum bone width of 6–7 mm, preserving the ridge is essential [5]. By anticipating these remodelling patterns, clinicians can apply targeted strategies to maintain ridge integrity.
Achieving the best results demands a combination of biological understanding and timely clinical action. By addressing site-specific needs and leveraging insights into bone remodelling, clinicians can protect the alveolar ridge, ensuring both functional stability and aesthetic restoration.
FAQs
How soon after an extraction does jawbone shrinkage start?
Jawbone shrinkage often starts as early as six weeks after a tooth is extracted. During this period, the bone can undergo noticeable resorption, potentially altering the shape and structure of the alveolar ridge.
Can ridge preservation prevent needing bone grafting later for implants?
Yes, ridge preservation can help maintain the volume of the alveolar bone, which may minimise or postpone the need for bone grafting when preparing for implants. However, it doesn’t entirely rule out the possibility of grafting, as factors like individual healing and the degree of bone loss play a significant role.
What health conditions can slow socket healing and bone regrowth?
Conditions like osteoporosis, diabetes, and other systemic illnesses can interfere with the healing of sockets and the regrowth of bone. These conditions affect bone metabolism and limit blood flow – both of which are essential for effective healing and regeneration.
Related Blog Posts
- Impact of Implantoplasty on Implant Fatigue Resistance
- 3D Bioprinting for Oral and Facial Tissue Repair
- Advances in Bone Grafting for Implant Stability
- Bone Graft Healing Stages Explained
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





