







Advances in Bone Grafting for Implant Stability

Dental implants depend on sufficient jawbone to stay stable. But when bone is lost – due to extractions, disease, or trauma – bone grafting becomes essential. Each year, 10.7 million dental implants are placed globally, with 25% requiring bone grafting. The grafting materials market exceeds $2.5 billion annually, reflecting the demand for effective solutions.
Here’s a quick breakdown:
- Bone Loss After Extraction: Up to 60% of bone volume can be lost in the first three months.
- Grafting Materials: Options include autografts (from the patient), allografts (human donors), xenografts (animal sources), and synthetic alloplasts.
- Techniques: Common methods include socket preservation, ridge augmentation, and sinus lifts.
- New Developments: Nanotechnology, 3D-printed scaffolds, and bioactive growth factors are improving outcomes.
These advancements are helping clinicians restore bone effectively, ensuring implants are stable and long-lasting.
Tooth Extraction and Bone Grafting for Dental Implants
Bone Grafting Materials
Comparison of Bone Grafting Materials for Dental Implants
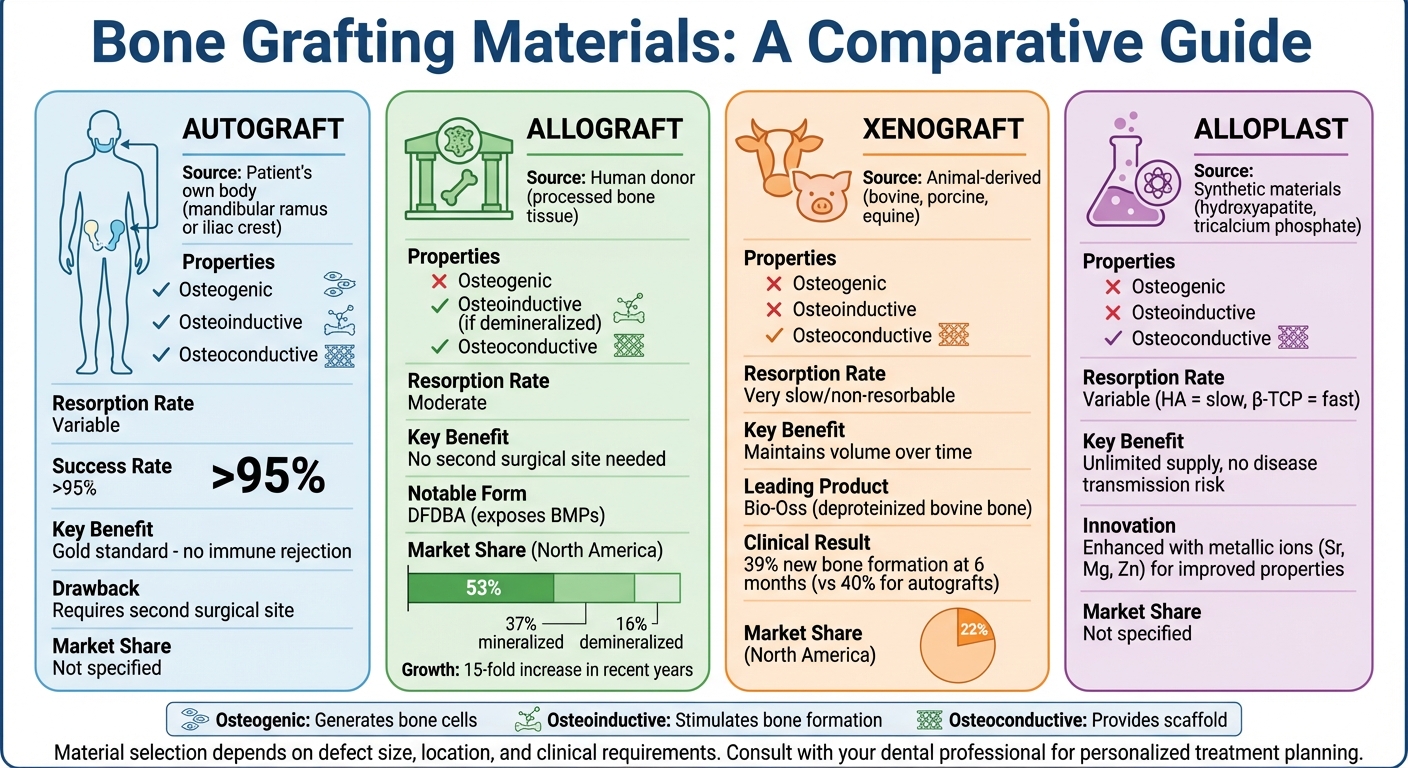
Selecting the right bone grafting material is crucial for the success of implants. The four main types – autografts, allografts, xenografts, and alloplasts – each have unique sources, resorption rates, and regenerative properties. The material chosen plays a significant role in osseointegration, which directly impacts the stability of the implant. Let’s take a closer look at the characteristics and clinical applications of each type.
Autografts are often considered the gold standard because they uniquely provide osteogenesis, osteoinduction, and osteoconduction [6][2]. Sourced directly from the patient, usually from the mandibular ramus or iliac crest, they eliminate the risk of immune rejection and boast a success rate exceeding 95% [4]. However, the need for a second surgical site can increase patient discomfort and extend recovery time.
Allografts, derived from human donors, remove the need for a second surgical site. In North America, mineralised forms account for 37% of procedures, while demineralised forms make up 16% [2]. Among these, Demineralised Freeze-Dried Bone Allografts (DFDBA) are particularly notable. The demineralisation process exposes bone morphogenetic proteins (BMPs), making them both osteoconductive and osteoinductive [2][8]. These BMPs play a key role in stimulating bone formation. Advancements in processing have led to a 15-fold increase in allograft use in recent years [9].
Xenografts, derived from animals such as bovines, porcine, or equine sources, are another option. The most widely used xenograft in clinical dentistry is Bio-Oss, a deproteinised bovine bone mineral produced by Geistlich in Switzerland [6]. These materials are treated at high temperatures to remove organic components, resulting in a product that is either non-resorbable or very slow to resorb. This makes them ideal for maintaining bone volume over time, especially in procedures like maxillary sinus augmentation and ridge preservation. Studies indicate that sinus sites grafted with Bio-Oss achieved 39% new bone formation after six months, closely matching the 40% observed with autografts [8]. Xenografts currently make up about 22% of the North American market [2].
Alloplasts, which are synthetic materials, offer an unlimited supply and eliminate concerns about disease transmission. However, they provide only osteoconduction [6][4]. Different types of alloplasts have varying resorption rates; hydroxyapatite resorbs slowly and provides long-term stability, while tricalcium phosphate resorbs more quickly and is replaced by natural bone at a faster rate. Recent advancements include the addition of metallic ions such as strontium, magnesium, and zinc to hydroxyapatite to enhance osteoinductive properties and antibacterial effects [6][3].
Below is a summary of the key attributes of these grafting materials:
| Material Type | Source | Osteogenic | Osteoinductive | Osteoconductive | Resorption Rate | Primary Benefit |
|---|---|---|---|---|---|---|
| Autograft | Patient’s own body | Yes | Yes | Yes | Variable | High success rate; no immune rejection |
| Allograft | Human donor | No | Yes (if demineralised) | Yes | Moderate | No need for a second surgical site |
| Xenograft | Animal (bovine/porcine) | No | No | Yes | Very slow | Maintains volume over time |
| Alloplast | Synthetic | No | No | Yes | Variable | Unlimited supply; no disease risk |
Common Bone Grafting Techniques
After selecting the suitable material, the next crucial step is determining the best technique to address the specific bone deficiency and implant location. Techniques like socket preservation, ridge augmentation, and sinus lifts are commonly used in dental implantology. Each method targets unique challenges to ensure there’s enough bone volume and stability for successful implants. These approaches range from minor procedures to more complex interventions, depending on the severity and location of the bone loss.
Socket Preservation
When a tooth is extracted, the surrounding alveolar bone naturally starts to shrink, losing 40%–60% of its volume [1]. Socket preservation is a procedure performed immediately after tooth extraction to prevent this collapse, maintaining the ridge’s shape for future implant placement.
In February 2019, Prof. Eli E. Machtei from the Rambam Health Care Campus in Israel conducted a study involving 33 patients who required tooth extractions. The research compared three groups: those who underwent socket preservation with biphasic calcium sulphate/hydroxyapatite (BCS/HA), those treated with bovine-derived xenograft (BDX), and a control group with no grafting. The control group experienced a significant ridge width reduction of 2.96 ± 0.3 millimetres, while the BCS/HA group saw a much smaller loss of just 0.5 ± 0.4 millimetres. This clearly shows how effective socket preservation is in maintaining ridge dimensions for future implants [10]. Typically, patients wait three to four months for the graft to integrate before proceeding with implant placement [14].
For more severe bone loss, socket preservation alone may not be enough, and ridge augmentation becomes necessary.
Ridge Augmentation
Ridge augmentation is used when there’s significant bone loss, restoring both the width and height of the ridge. This technique is essential when the bone is too narrow or shallow to securely hold an implant [1][5]. The most widely used method is Guided Bone Regeneration (GBR), which relies on barrier membranes to block soft tissue cells from invading the defect site. This allows bone cells, which regenerate more slowly, to repopulate the area [12][13]. GBR can be performed at the same time as implant placement for smaller defects or as a staged procedure for larger ones [12].
One retrospective multicentre study examined 123 implants placed in sites augmented with vertical GBR using non-resorbable membranes combined with autogenous bone chips or demineralised freeze-dried bone allografts. After one to five years of prosthetic loading, the implants showed a 97.5% success rate, proving that GBR-regenerated bone supports implants just as well as natural bone [1]. However, membrane exposure during healing can significantly reduce bone regeneration – by as much as 50% [1]. For vertical bone deficiencies, GBR is most effective for gains up to 4 millimetres. Larger defects typically require a staged approach [1].
Sinus Lifts and Guided Bone Regeneration (GBR)
In the upper back jaw, the proximity of the maxillary sinus to the ridge often leaves insufficient bone height for implant placement. A sinus lift increases the vertical bone height in this area [11][7]. There are two main approaches: the lateral window technique and the transcrestal technique. The lateral approach is more invasive but allows for greater bone height gain, while the transcrestal method is less invasive and offers a quicker recovery.
A randomised trial conducted in August 2025 compared these two methods, focusing on transcrestal sinus lifts using osseodensification versus the lateral window technique. The transcrestal group achieved a mean bone height gain of 5.33 ± 0.83 millimetres and an ISQ (implant stability quotient) of 80.00 ± 3.11, compared to the lateral group’s 10.02 ± 1.82 millimetres gain and 75.86 ± 2.91 ISQ. The results suggested that while the lateral technique provides greater bone height, osseodensification offers a less invasive option with excellent primary stability [11].
sbb-itb-2be92ed
Recent Research on Osseointegration and Implant Stability
Understanding how bone grafts merge with natural bone tissue is crucial for predicting the success of implants. Osseointegration – the direct connection between living bone and the implant surface – relies on a combination of factors working in harmony. Recent studies have explored how various graft materials impact this process and the recovery timelines that clinicians can realistically anticipate.
How Biomaterial Properties Affect Bone Integration
Bone regeneration is a complex process supported by six key elements: osteogenic cells, osteoinductive signals, osteoconductive scaffolds, mechanical stability, vascularisation, and a conducive host environment [6]. When any of these factors is compromised, the integration process may falter.
The chemical makeup of graft materials significantly influences how quickly and effectively new bone forms. For example, trace elements like Strontium (Sr²⁺) encourage osteoblast proliferation, while Zinc (Zn²⁺) enhances collagen production and increases alkaline phosphatase levels [3]. These additions transform graft materials from being merely structural supports to actively promoting bone growth.
Porosity is another critical factor. An optimal pore size – no less than 100 µm and ideally within the range of 300 µm to 1.2 mm – ensures proper vascularisation and osteogenesis [3]. Insufficient pore size or poor interconnectivity can hinder blood vessel growth, slowing down bone regeneration.
The rate at which graft materials resorb also needs to align with the natural pace of bone regeneration. For instance, β-tricalcium phosphate (β-TCP) resorbs within three to six months, while Hydroxyapatite (HA) and xenografts degrade more slowly, offering long-term volume stability but potentially delaying complete bone remodelling [6]. Biphasic calcium phosphates (BCP), which combine HA’s stability with β-TCP’s resorbability, provide a balanced degradation rate that can be tailored to suit individual healing needs [3].
A February 2024 randomised study conducted by Seoul National University Dental Hospital and Hallym University Sacred Heart Hospital highlighted these principles in a clinical setting. Researchers examined 60 patients undergoing guided bone regeneration, comparing customised 3D-printed ceramic bone grafts (OSTEON 3D) with conventional graft blocks. The 3D-printed grafts demonstrated higher bone volume (BV/TV) percentages and enabled successful implant placement approximately five months after grafting. Additionally, the precise fit of the 3D-printed grafts reduced surgical time [15]. These material-specific benefits contribute to the consistently high implant survival rates observed in practice.
Clinical Success Rates and Recovery Timelines
The properties of these biomaterials play a direct role in achieving high clinical success rates and predictable recovery timelines. Evidence from clinical studies shows that bone graft-supported implants have survival rates exceeding 97% across various grafting methods [1][16].
"The implant survival rate does not differ between the two types of bone graft in a guided bone regeneration or in an autogenous bone block" [16].
Recovery follows a predictable timeline. Bone mineralisation begins around 30 days after grafting and is typically completed by 90 days in trabecular bone and 130 days in cortical bone [6]. Synthetic β-TCP granules achieve full resorption and integration within three to six months after implantation [6].
These materials’ effectiveness is reflected in consistent implant survival rates and rapid bone integration. Studies show that synthetic biomaterials preserve 85–95% of bone volume, comparable to traditional xenografts [17]. Additionally, combining rhBMP-2 with β-TCP boosts new bone formation to 21.18% ± 7.62%, compared to 13.44% ± 6.03% with β-TCP alone [17]. These advancements could potentially shorten treatment times by accelerating graft site maturation.
New Developments in Bone Regeneration
Advancements in bone grafting technology are transforming the field, making procedures faster, simpler, and more predictable. These innovations build on earlier breakthroughs in graft materials and surgical techniques, further enhancing implant stability.
Nanotechnology in Bone Grafting
Nanotechnology has introduced grafts engineered at scales smaller than 100 nanometres, designed to replicate the natural structure of bone [2][6]. This precise design increases the surface area for cellular interactions, boosting bioactivity and speeding up the resorption process [3].
"Today, many bone-grafting materials have been designed with specific surface topographies at both the micro- and nanoscales to further guide new bone formation once implanted in situ." – Richard J. Miron, Department of Periodontology, University of Bern [2]
Nanocrystalline grafts not only release calcium quickly but also incorporate elements like Strontium, Magnesium, and Zinc. These elements stimulate bone growth signals and provide antibacterial benefits [3][6]. For example, a 2025 clinical study highlighted the effectiveness of Ostim®, a nanocrystalline hydroxyapatite product, in promoting early epithelialisation by day 7. It also activated key markers like VEGF and IL-10, achieving faster biological integration compared to traditional grafting materials [17]. These advancements in nanostructured grafts are opening doors for creating highly customised scaffolds.
3D Printing for Custom Scaffolds
3D printing has taken bone grafting to the next level by enabling the creation of scaffolds tailored to fit specific defect sites. With CAD/CAM technology, clinicians can design scaffolds that perfectly align with the host bone, reducing the need for manual adjustments during surgery and cutting down on operative time [15][6][18].
In February 2024, a study published in Scientific Reports examined OSTEON 3D, a 3D-printed ceramic bone graft by Dentium (Seoul, Korea). The study involved 60 patients undergoing guided bone regeneration for dental implants. Results showed the 3D-printed grafts achieved a significantly higher bone volume (BV/TV) compared to conventional block grafts, while also reducing surgery time and patient discomfort [15].
These 3D-printed scaffolds are designed with interconnected pores larger than 100 microns, which promote faster vascular growth [18][19]. Researchers Wu et al. even applied Voronoi-Tessellation principles to create ceramic maxillofacial prostheses with gradient pore structures. This design reduced peak mechanical stress by approximately 46% compared to traditional uniform scaffolds, highlighting the potential of customised designs [18].
Growth Factors for Faster Bone Formation
The integration of bioactive growth factors into grafting techniques is another game-changer. These factors act as biological signals, guiding progenitor cells to become bone-forming osteoblasts. Among these, Bone Morphogenetic Protein-2 (BMP-2) is the most widely studied. In North America, recombinant human BMP-2 (rhBMP-2) is used in about 5% of bone augmentation procedures [2]. When paired with synthetic scaffolds, BMP-2 can significantly speed up bone formation.
For instance, a clinical study by Sun Y et al. demonstrated that combining rhBMP-2 with BioCaP and β-TCP produced a new bone area of 21.18% ± 7.62%, compared to 13.44% ± 6.03% with β-TCP alone [17].
Delivery methods also play a crucial role. In an ovine extraskeletal model, Moussa et al. tested a 3D-printed bio-ceramic scaffold loaded with 100 µg of rhBMP-2. At 16 weeks, the BMP-2–loaded scaffold showed significantly higher bone formation and nearly complete degradation, outperforming scaffolds without BMP-2 [19]. This highlights the powerful synergy between advanced scaffolds and bioactive agents, accelerating both bone regeneration and graft integration.
Conclusion
Bone grafting techniques have come a long way, offering a variety of methods to improve the stability of dental implants. From traditional autografts to cutting-edge nanotechnology materials and tailored 3D-printed scaffolds, these advancements are making it easier to mimic the body’s natural bone regeneration processes.
One of the key frameworks driving this progress is the Diamond Concept. This approach highlights six critical components for successful bone regeneration: osteogenic cells, osteoinductive signals, osteoconductive scaffolds, mechanical stability, vascularisation, and a supportive host environment [6]. When these elements align, research indicates that synthetic biomaterials can preserve bone at rates of 85% to 95%, rivaling the effectiveness of traditional xenografts [17].
"Selecting defect-specific regenerative approaches is crucial for successful outcomes in alveolar bone augmentation." – Ahmed Yaseen Alqutaibi, Researcher [1]
Modern bone grafting also emphasises personalised treatment plans. Using tools like the CCARD classification system and decision trees, practitioners can adapt their methods to fit each patient’s unique anatomy and health profile [1]. This tailored approach, paired with careful material selection, ensures more reliable and consistent results.
With advancements in growth factors, nanotechnology, and 3D printing on the horizon, bone grafting is set to become even more efficient, paving the way for better implant success and improved patient care.
FAQs
What are the latest developments in bone grafting materials for improving dental implant stability?
Recent developments in bone grafting materials are steering toward smarter, bioactive solutions that improve the stability of dental implants. Scientists are now crafting biomimetic and synthetic materials that mimic the properties of natural bone, helping implants integrate more seamlessly and speeding up the healing process. These materials often include micro- and nanostructures that guide and support bone regeneration with greater precision.
On top of that, there’s growing interest in grafts enhanced with growth factors and peptide-functionalised biomaterials. These advancements are designed to encourage bone formation while keeping side effects to a minimum. The goal is clear: improve success rates for implants, reduce the reliance on donor site grafts, and ensure long-term stability for patients undergoing dental implant procedures.
How do bone grafting techniques improve the stability of dental implants?
Bone grafting techniques are essential for improving dental implant stability by addressing areas with insufficient bone. Procedures like guided bone regeneration (GBR), sinus lifts, socket preservation, and ridge augmentation are customised to rebuild bone structure, ensuring a solid base for implants.
These methods rely on different graft materials, including autografts, allografts, xenografts, and synthetic options. These materials support bone regrowth by offering the necessary framework for new bone to form. Advances such as growth factor-enriched grafts and tissue engineering have further refined these techniques, boosting implant success rates and ensuring long-term durability.
For those considering dental implants, consulting a skilled dental professional is key to finding the approach that best suits your specific needs.
How does nanotechnology improve bone grafting for dental implants?
Nanotechnology is transforming the field of bone grafting by boosting both the biological and mechanical qualities of graft materials. With nano-engineered materials, the structure closely resembles natural bone, which encourages better cell attachment, growth, and regeneration. As a result, these materials often outperform traditional options in aiding bone healing and integration.
One of the standout features of nanotechnology in this context is its ability to deliver growth factors and bioactive molecules in a controlled manner. By releasing these substances gradually at the graft site, it ensures they remain effective for longer, avoiding premature breakdown. This precise delivery system plays a key role in supporting consistent bone regeneration. These advancements not only enhance the stability of bone grafts but also improve the overall success rates of dental implants.
Related Blog Posts
- How Hybrid Coatings Improve Osseointegration
- Osseointegration in Titanium Implants: How It Works
- Surface Modifications for Better Osseointegration
- Bone Quality in Osseointegration: Research Insights
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





