







Challenges in Dental 3D Bioprinting
3D bioprinting is reshaping dental care by enabling the creation of living tooth structures. Unlike traditional implants, this technology aims to restore biological function. However, it’s far from ready for widespread clinical use. Key challenges include:
- Material Limitations: Issues like biocompatibility, mechanical weaknesses, and degradation in the oral environment hinder progress.
- Technical Precision: Printing accuracy, surface quality, and replicating complex tooth structures remain problematic.
- Costs and Accessibility: High equipment and material costs limit adoption, especially in rural areas.
- Regulatory and Training Barriers: Unclear regulations and lack of training slow clinical implementation.
Despite these obstacles, advancements in bioinks, AI integration, and regulatory clarity are helping to address these issues. Continued collaboration between researchers, clinicians, and regulators is crucial for progress.
Material Limitations in Dental 3D Bioprinting
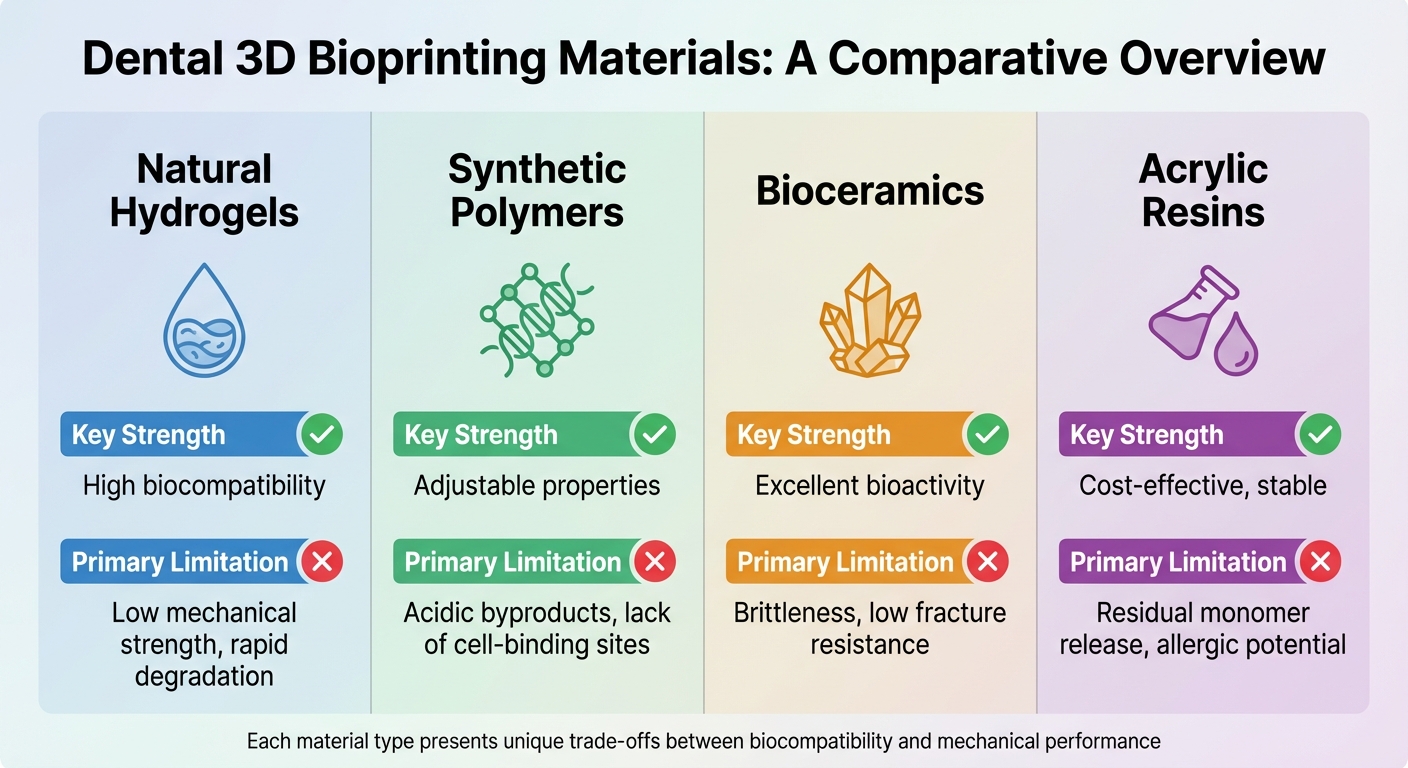
Comparison of Dental 3D Bioprinting Materials: Strengths and Limitations
When it comes to dental 3D bioprinting, the materials themselves present significant hurdles. Everything from biocompatibility and safety concerns to mechanical weaknesses complicates their use in clinical settings. These material-related challenges often snowball into broader technical and financial obstacles.
Biocompatibility and Durability Problems
A key issue with dental 3D printing materials is residual monomer toxicity. During the printing process, incomplete polymerisation can leave behind harmful substances like methyl methacrylate, which has been linked to mucosal irritation, allergic reactions, and pulp damage [6]. Researchers from MDPI explain:
"Three-dimensional printing generates the release of residual monomers due to incomplete polymerisation of materials and involves the use of potentially toxic substances in post-printing processes that cannot be completely eliminated." [6]
Another major concern is the mismatch in mechanical properties. Natural hydrogels, often the base for bioinks, lack the strength required to replicate the load-bearing nature of dental tissues. For instance, dentin has a Young’s modulus ranging from 17 GPa near the pulp to 42 GPa in central areas, while high-density alveolar bone measures around 13.7 GPa [3]. In comparison, bioceramics, though bioactive, are brittle with poor fracture and flexural resistance [1].
Synthetic polymers like PLA and PLGA add to the complexity. They degrade into acidic byproducts, which can trigger inflammation [1]. Meanwhile, materials such as alginate and PCL fail to provide essential cell-anchoring sites (RGD motifs), requiring extra modification to support cell attachment [1]. The oral environment itself – packed with salivary enzymes, bacteria, and constant temperature changes – further accelerates degradation and structural distortion of bioprinted constructs [6][7].
Current Bioink Limitations
On top of these issues, bioinks face additional challenges, particularly when it comes to mimicking natural vascularisation and synchronising degradation rates. Vascularisation – the intricate network of blood vessels needed for dental pulp and bone to function properly – remains a significant hurdle [3]. For example, natural dental pulp has a storage modulus of about 100 Pa, but many collagen-based bioprinted constructs reach around 280 Pa, failing to replicate the original tissue accurately [3].
Another sticking point is degradation synchronisation. For successful tissue regeneration, scaffolds must degrade at the same rate that cells produce new extracellular matrix (ECM). If the timing is off, the structure may either collapse too early or linger too long, disrupting tissue integration [3]. This is especially critical given that periodontitis, a condition affecting nearly half of the population, requires precise material performance [3].
These material challenges highlight the broader mechanical and biological barriers in advancing dental 3D bioprinting.
| Material Type | Key Strength | Primary Limitation |
|---|---|---|
| Natural Hydrogels | High biocompatibility | Low mechanical strength, rapid degradation [3][1] |
| Synthetic Polymers | Adjustable properties | Acidic byproducts, lack of cell-binding sites [1] |
| Bioceramics | Excellent bioactivity | Brittleness, low fracture resistance [1] |
| Acrylic Resins | Cost-effective, stable | Residual monomer release, allergic potential [6][7] |
sbb-itb-2be92ed
Technical and Precision Challenges
Creating clinical-grade dental restorations is no small feat. The process is riddled with challenges, from the limitations of materials to the technical precision required. One of the primary hurdles lies in the layer-by-layer construction methods used in 3D printing, which struggle to meet the exacting standards needed for dental applications. The intricate geometry of teeth only adds to the complexity.
Printing Accuracy and Surface Quality
The layer-by-layer technique often leads to what’s called the "stair-step" effect – those tiny ridges that form on a printed surface. This isn’t just an aesthetic issue; it can affect patient comfort and even encourage plaque build-up. Yasaman Etemad-Shahidi from Griffith University‘s School of Dentistry and Oral Health explains:
"Models acquired through vat polymerisation and material jetting are prone to shrinkage during the polymerisation stage as well as having stair-step surfaces due to the layering technique used in construction." [8]
Another major issue is polymerisation shrinkage, which happens during UV curing. This contraction can cause dimensional errors that exceed clinical tolerances. And it doesn’t stop there – these dimensional changes can continue to develop weeks after the initial manufacturing. Research shows that errors can range from as small as 3.3 μm to over 500 μm [8]. To put that in perspective, fixed prosthodontics require errors to stay below 0.2 mm to be considered clinically acceptable [9].
Smaller nozzles can help achieve finer detail, but they come with their own set of trade-offs, including higher shear stress. This stress can damage cells or reduce their bioactivity, especially in bioinks, which are often hydrogel-based and lack the mechanical strength needed for functional dental tissues [1][3]. For example, while pulp-like constructs have a strength of about 0.8 kPa, natural dentin boasts a Young’s modulus ranging from 17 GPa near the pulp to 42 GPa in other regions [3].
Recreating the tooth’s complex, layered structure is another significant challenge. Fengxiao Zhao from the State Key Laboratory of Oral Diseases highlights this difficulty:
"The natural tooth features a sophisticated and hierarchically organized architecture. Given that, the reproduction of complicated structure and integrated complex tissue remain challenging." [1]
For instance, regenerating dentin requires pores around 300 μm in size to allow odontoblasts to extend their cytoplasm properly [3]. The post-processing steps, like cleaning with isopropyl alcohol and additional UV curing, can also cause further material shrinkage, complicating matters even more [8][9].
And beyond just the surface, the complex anatomy of teeth – especially the biting surfaces – introduces functional challenges.
Occlusion and Functionality Requirements
The occlusal surfaces of teeth, with their deep pits and grooves, are particularly tricky to replicate accurately. These areas are prone to trapping adhesive or uncured resin, which can harden over time and distort the fit [11]. Posterior teeth, with their intricate pits and fissures, often show deviations exceeding 0.1 mm. This can lead to marginal leakage, compromising the restoration’s longevity [11].
For full-arch models, trueness values typically range from 73.9 to 194 μm [9]. Achieving the precision needed for proper mastication and speech requires careful attention to internal structures, including porosity and pore shapes. These details are critical for mechanical stability, especially in load-bearing areas that endure daily chewing forces [4].
These challenges go beyond aesthetics – they directly impact the functionality and durability of dental restorations. The technical demands of achieving both accuracy and stability make the entire process a complex balancing act.
Economic and Accessibility Barriers
The financial challenges tied to dental 3D bioprinting are a significant hurdle. For many dental practices – especially smaller clinics and those in regional areas – the upfront costs are prohibitive. These financial pressures compound the technical difficulties already discussed, creating a layered barrier to adopting this technology in clinical settings.
High Equipment and Material Costs
The cost of bioprinting equipment varies widely depending on the technology. Laser-assisted methods like SLA, DLP, and SLS provide exceptional precision and speed but come with steep price tags compared to simpler systems [2][1]. Entry-level bioprinters, such as the Tissue Scribe, start at around A$1,500, while mid-range models like the Lulzbot Bio are priced at roughly A$10,000 [15]. However, professional-grade automated systems can climb well beyond A$1 million [15].
Material costs add another layer of expense. Unlike standard 3D printing filaments, bioinks are far more complex, as they must include living cells and bioactive agents [2][1]. Specialised materials like dECM and TDM require extensive processing, which drives up their cost [2][1]. Additionally, incorporating bioactive additives such as bone morphogenetic protein (BMP) peptides or growth factors like FGF-2 further inflates expenses. Reinforcing natural hydrogels with bioceramics or synthetic polymers to achieve the necessary mechanical properties adds yet another cost burden [2][1].
These high costs disproportionately impact clinics in rural or less densely populated areas, where budgets are often tighter.
Limited Access in Rural Areas
The distribution of dental practitioners in Australia reveals a stark imbalance. About 82.1% of dentists work in metropolitan areas, while only 0.1% serve very remote regions [14]. Tasmania, for instance, has just 26.5 dental practitioners per 100,000 residents compared to the national average of 72.5 per 100,000 [14].
For rural clinics, the sparse population and long travel distances make investing in advanced equipment like 3D bioprinters difficult to justify. These clinics often cater to low-income communities that cannot afford the higher costs associated with cutting-edge technology. Infrastructure challenges, such as unreliable internet connections, further complicate the adoption of digital imaging and teledentistry platforms – both of which are essential for efficient 3D printing workflows. Additionally, rural providers frequently lack access to the hands-on training required to operate these complex systems [13].
Despite these challenges, there are promising developments. The University of Queensland‘s Centre for Orofacial Regeneration, Reconstruction and Rehabilitation (COR3), under the leadership of Professor Saso Ivanovski, is working with the Herston Biofabrication Institute to create cost-effective, scalable 3D-printed scaffolds. Professor Ivanovski explains:
"COR3 has a goal for advancements to be cost-effective and scalable, ensuring the practical outcomes are disseminated broadly through public and private health services."
Government-led initiatives like the Stronger Rural Health Strategy aim to address workforce imbalances in regional areas, while community service grants provide funding for oral health projects in high-need locations [17].
Regulatory and Training Challenges
The rise of dental 3D bioprinting comes with its own set of hurdles, particularly in navigating regulations and addressing training gaps. As technology evolves faster than the rules governing it, uncertainty looms over how bioprinted dental constructs should be classified – are they medical devices, biologicals, or a mix of both? [18][21] This lack of clarity makes it tough for dental practices to ensure compliance. Adding to the complexity is the shortage of adequate training, which slows down clinical adoption.
Regulatory Uncertainty
Since February 2021, the Therapeutic Goods Administration (TGA) has tightened its oversight on dental 3D printing. Many personalised dental prints, once considered "custom-made", are now classified as "patient-matched medical devices" (PMMDs). These devices must be listed in the Australian Register of Therapeutic Goods (ARTG) by 1 July 2029 [19][21].
This change brings new responsibilities for dental professionals. For instance, dentists importing bioprinting materials like resins or bioinks from overseas automatically become the "sponsor" of those materials in Australia. This means they are legally responsible for ensuring ARTG compliance and reporting any safety issues [20].
There is, however, a "low volume exemption" for manufacturers who provide five or fewer patient-matched devices of a particular kind per financial year. While this allows them to skip ARTG inclusion, they must still adhere to the "Essential Principles" for safety and maintain detailed documentation, including adverse event reporting to the TGA [19][20]. Tajanka Mladenovska from St Vincent’s Hospital explains the regulatory challenge:
"The advent of such ‘mass-customised’ medical devices presents a major challenge for regulators as the current regulatory frameworks are designed for mass-manufactured, standardised products" [21].
Training Gaps for Dental Professionals
Even with cutting-edge equipment and clearer regulatory pathways, many dental practices face a major obstacle: a lack of skilled personnel. Traditional dental education hasn’t kept pace with the shift toward digital workflows, leaving professionals underprepared for integrating 3D bioprinting into their practice. The Australian Digital Dentistry Academy (ADDA) highlights this gap, focusing on practical, hands-on training rather than outdated classroom theories:
"Our philosophy centres around skill-sharing and practical knowledge rather than just classroom theory and certificates" [22].
For training to be effective, it must cover every stage of the digital workflow. This includes advances in intraoral scanning, CAD design, printing, post-processing, and even troubleshooting. It’s not just dentists who need this knowledge – dental assistants and practice managers must also be equipped to support these workflows [23][24][25]. The Institute of Digital Dentistry underscores the urgency:
"The hard truth is that in order to maintain an efficient practice, you have to utilise new technology as it becomes available. Otherwise, you’re offering suboptimal care" [24].
To address these challenges, some organisations now provide in-practice mentorship. Experts visit clinics to help teams quickly integrate 3D printing workflows. This hands-on approach ensures that practices can overcome practical barriers, which theoretical training alone often fails to address [25].
Current Solutions and Advancements
Despite the challenges, dental 3D bioprinting is steadily evolving, thanks to breakthroughs in materials science, artificial intelligence, and regulatory frameworks. These developments aim to address earlier limitations, making the technology more practical and accessible.
Advances in Bioinks and Printing Materials
The development of bioinks has seen exciting progress, blending natural and synthetic materials to achieve both biological compatibility and mechanical durability. For example, incorporating nanohydroxyapatite (nHA) into alginate‐gelatin matrices has been shown to mimic the mineral phase of bone. This not only strengthens the hydrogel but also enhances the stability of printed structures [26]. In January 2026, researchers Nikos Koutsomarkos and Maria Chatzinikolaidou from the University of Crete created composite bioinks with various nHA concentrations. Their 4% nHA formulation demonstrated promising results in terms of viscosity recovery and cell viability [26].
Treated dentin matrix (TDM) bioinks are another advancement, releasing biomolecules to foster dentin regeneration. Similarly, gelatin methacryloyl (GelMA) bioinks, enhanced with peptides, promote differentiation of tooth cells [1]. Hybrid bioinks combining natural polymers like collagen with synthetic materials such as polycaprolactone (PCL) or bioceramics like beta‐tricalcium phosphate (β‐TCP) are gaining attention for balancing biological signalling with the strength required for hard tissue applications [1][10][27]. A notable milestone came in February 2023, when Alghadeer and colleagues successfully created human enamel organoids using induced pluripotent stem cells, producing a mineralised enamel matrix. This marks a significant step toward growing functional enamel in the lab [27]. As Luca Fiorillo from the University of Enna "Kore" explains:
"The integration of digital dentistry, bioprinting, and stem cell science points toward future ‘grow and glue’ restorations that may replace traditional drill-and-fill methods"
[27].
AI Integration for Precision and Efficiency
Artificial intelligence is revolutionising dental bioprinting by automating and optimising various processes. AI algorithms can convert medical imaging into precise 3D models with minimal manual input [28]. Machine learning further refines the process by predicting the best bioink formulations, taking into account factors like printability and biocompatibility. Real-time monitoring systems powered by AI can also adjust printing parameters on the fly, ensuring high precision and reducing errors [28]. Jie Huang highlights this transformative potential:
"AI can automate these processes to achieve more consistent and precise outcomes, reducing human error and increasing efficiency"
[28]. These advancements are especially crucial for complex dental structures, where accurate cell placement and material deposition are essential. There’s also growing interest in in situ bioprinting, where tissues are printed directly inside a patient’s mouth during surgery, with AI assisting in the process [28]. Such innovations align with regulatory advancements, paving the way for broader clinical adoption.
Regulatory Progress and Training Programs
Regulatory frameworks are adapting to keep pace with the growth of dental bioprinting. Updated TGA guidelines, effective from 13 January 2026, provide clearer legal requirements for dental practitioners involved in importing or manufacturing 3D-printed devices [29]. The shift from a broad "custom-made" exemption to a more specific "patient-matched medical device" (PMMD) framework means most 3D-printed dental constructs now require conformity assessment and inclusion in the Australian Register of Therapeutic Goods (ARTG) [30]. For instance, if a dentist imports a new resin from an overseas supplier, they must ensure the material is listed in the ARTG and meet all sponsor obligations, including adverse event reporting [30]. Elexes Medical Consulting underscores the importance of understanding these responsibilities:
"The January 2026 guidance reinforces that misunderstanding sponsor roles is not an acceptable defence"
[29].
To ease the transition, PMMDs notified to the TGA before 1 November 2024 can continue to be supplied without ARTG inclusion until 1 July 2029, giving practitioners time to adapt [30]. These regulatory updates, coupled with training programs, aim to address barriers to adoption and ensure a smoother integration of this cutting-edge technology into clinical practice.
Conclusion
Dental 3D bioprinting holds exciting potential for regenerative dentistry, but there are still obstacles to overcome before it becomes a standard part of clinical practice. One of the biggest challenges lies in replicating the complexity of dental tissues, especially the dentoalveolar system, which is a unique combination of nerves, ligaments, enamel, and bone [3].
On the technical side, production efficiency remains an issue. Creating intricate dental structures with high resolution demands a careful balance between speed and precision [1][5]. Financial barriers also play a role, with the high costs of equipment and specialised bioinks making it difficult for smaller practices to adopt this technology [5][12].
However, progress is being made. Hybrid bioinks are improving both bioactivity and mechanical stability [1][2]. Advances in digital planning, such as CBCT and CAD/CAM technologies, are enabling more precise surgical guides, which can lead to shorter surgeries and better patient outcomes [5][12]. As one study highlights:
"Accuracy, affordability, and professional recommendations are primary criteria influencing the adoption of 3D printing among dentists, dental technicians, and CAD/CAM experts" [5].
With the support of evolving regulations, new training programs, and AI-driven workflows, dental bioprinting is steadily moving from experimental stages to practical applications. Continued collaboration between material scientists, clinicians, and regulators will be essential to ensure this technology delivers safe and effective results for patients.
FAQs
When will bioprinted teeth be available in Australia?
Bioprinted teeth are expected to hit the Australian market by 2026, coinciding with the rapid growth predicted for the global dental 3D printing industry during that time. These advancements promise to transform dental care, offering new and advanced options for tooth replacement and restoration.
What makes a bioprinted tooth safe to use in the mouth?
Bioprinted teeth can be safely used in the mouth when crafted from carefully chosen materials, like bioinks made with biocompatible and non-toxic cells and biomaterials. To ensure safety, these materials undergo thorough biological testing, including both in vitro (lab-based) and in vivo (animal or human-based) assessments. This rigorous process helps confirm that the materials won’t trigger harmful reactions or toxicity, making them fit for dental use.
Will dental 3D bioprinting make treatment cheaper in the long run?
Dental 3D bioprinting is shaping up to be a game-changer in reducing treatment costs over time. Take 3D-printed dental implants, for instance – they often come at a fraction of the price compared to traditional methods. Beyond cost savings, this technology speeds up procedures, shortens surgery times, and cuts down on material waste. The result? Fewer trips to the dentist and lower overall expenses. While the upfront investment in equipment is steep, the efficiency and ability to customise treatments could make dental care much more budget-friendly in the long run.
Related Blog Posts
- 3D Bioprinting in Dental Implants: How It Works
- 3D Printing in Dental Implant Prototyping: How It Works
- How 3D Bioprinting Creates Periodontal Scaffolds
- Emerging Trends in 3D-Printed Dental Prosthetics
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





