







Advances in Biomimetic Dental Surgery Materials

Biomimetic dental materials are reshaping how damaged teeth are restored by closely imitating the natural structure and function of enamel, dentin, and other tooth components. Unlike traditional methods that often involve removing healthy tooth structure, biomimetic techniques focus on preserving and rebuilding teeth with restorative material options that act like natural tissues.
Here’s what you need to know:
- What are biomimetic materials? These are materials designed to mimic the mechanical and biological properties of real teeth, promoting natural-like function and appearance.
- Key innovations:
- Enamel analogues are now 3.4 times tougher than natural enamel.
- Polydopamine adhesives offer stronger bonds in the moist oral environment.
- Self-healing composites automatically repair cracks.
- 3D printing enables precise, patient-specific restorations.
- Why it matters: Biomimetic solutions reduce the need for invasive procedures, preserve more of your natural tooth, and offer longer-lasting results compared to conventional materials.
- Challenges: Current limitations include high costs, complex manufacturing, and the need for more long-term clinical studies.
These advancements are changing dental care, offering less invasive and more effective options for tooth restoration. However, further research and cost reductions are needed to make these solutions more accessible.
An introduction to Biomimetic Dentistry
sbb-itb-2be92ed
Recent Advances in Biomimetic Dental Materials
Recent breakthroughs in dental materials have focused on improving three main areas: stronger bonding techniques, composite materials that better mimic natural tooth structure, and advanced 3D printing technologies for precise, patient-specific restorations. These developments are reshaping the field of dentistry by offering more durable and personalised solutions.
Adhesive Protocols and Bonding Techniques
Modern bonding methods now achieve chemical bonds that rival the strength of natural teeth. One example is the semi-direct bulk filling technique, which combines elements of both direct and indirect approaches. By curing a composite block outside the mouth before reinserting and bonding it, this method reduces polymerisation shrinkage stress. It achieves a tensile bond strength of 51.1 ± 12.2 MPa – a 58% improvement over traditional direct bulk fillings (32.4 ± 8.2 MPa) – and closely matches the natural dentin–enamel junction’s strength of 46.9 to 51.5 MPa [7].
Another exciting material is polydopamine (PD), inspired by the adhesive proteins found in mussels. PD replicates the DOPA motif from mussel foot proteins, enabling strong "wet adhesion" in the moist oral environment. Research shows PD bonds more effectively to enamel than conventional glass ionomer cement, with fewer microcracks at the interface [8]. According to Yao, C. et al. [8]:
"The wet bio-adhesive capacity, inhibitory effect on Matrix-metalloproteinases (MMP), and biomimetic remineralisation capabilities render PD a valuable additive for dental adhesives."
The immediate dentin sealing (IDS) technique has also become a key biomimetic practice. By applying an adhesive agent to freshly cut dentin before taking impressions, IDS protects the dentin–pulp complex while enhancing bond strength [4]. Refinements to this method, such as adding a thin (0.5 mm) layer of flowable composite over the adhesive, help ensure full polymerisation of the adhesive resin [7].
These advancements in bonding pave the way for more effective and durable composite materials.
New Developments in Composite Materials
Recent composite materials are designed to better replicate the mechanical properties of natural teeth. For example, short fibre-reinforced composites like EverX Flow act as a barrier against crack propagation, mimicking the fibrous structure of the dentin–enamel complex [3]. These materials are often used in a bilayered design, with a tough fibre-reinforced base supporting a wear-resistant, polishable surface composite – providing durability and stress distribution similar to natural teeth.
Self-healing composites are another innovation. These materials contain microcapsules that release healing agents when cracks form, sealing defects automatically. When combined with bioactive glass and calcium phosphate, they chemically bond to tissues and encourage the remineralisation of surrounding dentin [3][11].
Nanohybrid composites, which incorporate silica nanoparticles, offer improved polishability, translucency, and wear resistance. Additionally, using the semi-direct technique with these materials can reduce restoration time by nearly 60% (approximately 4.5 minutes) compared to traditional incremental layering methods [7].
These advanced composites work hand-in-hand with digital fabrication techniques, particularly 3D printing.
3D Printing Applications in Biomimetic Dentistry
3D printing has revolutionised dentistry by enabling the creation of highly accurate dental replicas. In May 2022, researchers at Queen Mary University of London developed biomimetic typodont teeth using Digital Light Processing (DLP) 3D printing. By incorporating 25 wt. % hydroxyapatite (HAp) and carbonated hydroxyapatite (CHAp) into a methacrylate-based photopolymer resin, they replicated the 0.31 N cutting force characteristic of natural enamel. X-ray microtomography (XMT) was used to map tooth geometry at a 15 μm voxel size, resulting in artificial teeth that provide realistic tactile feedback for dental training [9][12].
Beyond training, 3D bioprinting is being explored in regenerative dentistry to create scaffolds for pulp and dentin–pulp complex regeneration, encouraging both angiogenesis and neurogenesis [4][3]. CAD/CAM systems combined with 3D printing allow for patient-specific restorations that mimic the hierarchical structure of natural tooth enamel [2].
However, while 3D printing offers exceptional accuracy and customisation, milled nanohybrid composites still outperform 3D-printed materials for permanent restorations. For instance, milled composites exhibit significantly higher flexural strength (247.7 ± 29.1 MPa) compared to 3D-printed versions (97.2 ± 10.2 MPa) [10].
Techniques for Dentin Remineralisation
Recent advancements in bonding and composite materials have paved the way for remineralisation methods that focus on rebuilding tooth structure instead of merely replacing it. These techniques offer a fresh perspective on tackling early decay.
Self-Assembling Peptides for Remineralisation
P11-4, marketed as Curodont Repair™, has shown promise in addressing early carious lesions. This self-assembling peptide works by penetrating these lesions and forming a 3D β-sheet scaffold when exposed to a pH below 7.4 and in the presence of cations [13][14][15]. The peptide’s glutamate residues attract calcium and phosphate ions, creating sites for mineral growth.
Clinical trials have highlighted the efficacy of P11-4 in treating initial, non-cavitated lesions. Mohammad Alkilzy from the Department of Preventive and Paediatric Dentistry noted:
"The size of early carious lesions treated with P11-4 was significantly reduced, and this reduction was superior to that achieved with fluoride varnish treatment" [14].
Approximately 35% of the applied P11-4 remains in the lesion, forming a regenerative scaffold. However, its application is mostly limited to accessible occlusal or buccal lesions [14][18]. Proper surface preparation is crucial for success – this involves cleaning with sodium hypochlorite (NaOCl) and lightly etching with phosphoric acid to remove the hypermineralised surface layer before application [13][18].
Another promising technique, the PILP system, offers a different pathway for restoring demineralised dentin at the nano-scale.
Polymer-Induced Liquid Precursor (PILP) Systems
The PILP system takes a unique approach to remineralisation. Instead of relying on existing seed crystallites for mineral growth, it uses a particle-based method. Biomimetic compounds, such as polyacrylic acid (PAA) or polyaspartic acid (PASP), gather ions into 10–50 nm amorphous calcium phosphate (ACP) nanoprecursors [17]. These precursors remain in a liquid-like state, allowing them to penetrate the microscopic spaces within dentin collagen fibrils. Once inside, they mature into hydroxyapatite crystals, effectively restoring the collagen matrix.
A study published in Dental Materials in November 2020 demonstrated the potential of this approach. Artificial caries lesions, around 150 ± 50 μm thick, were treated with a high-concentration Ca/P-PILP solution over 20 days. The results showed an 88.0% remineralisation intensity, along with significantly improved micro-tensile bond strength and interfacial integrity compared to untreated samples [16]. PILP systems have even been shown to remineralise completely demineralised dentin lesions up to 250–300 μm thick, with some models achieving mineral densities close to 90% of the original enamel [14][17]. As noted in Pocket Dentistry:
"This bottom-up remineralisation strategy does not rely on seed crystallites, and may be considered as a potentially useful mechanism in extending the longevity of resin–dentin bonds" [17].
Comparing Biomimetic and Conventional Materials
Biomimetic vs Conventional Dental Materials: Key Differences and Performance Metrics
Looking at these materials side by side makes it clear why preserving natural tooth structure is so important. Conventional methods often follow the "extension for prevention" philosophy, which involves removing not just diseased tissue but also healthy tooth material to fit rigid, non-adaptive materials [3]. As Singer L, Fouda A, and Bourauel C put it:
"In conventional extension for prevention approach, not only the diseased but also sound tooth structure are removed and replaced with rigid, non-responsive materials. This treatment plan usually weakens the remaining tooth structure" [3].
This weakening of the tooth is a significant drawback. Biomimetic materials, on the other hand, focus on reducing stress and improving bonding, helping to maintain the tooth’s natural strength and integrity rather than compromising it through excessive preparation [3][4].
Key Differences in Structure and Function
Natural teeth are anisotropic, meaning their properties vary depending on the direction. Enamel is made up of intricate "fish scale" prisms, while dentin contains a collagen-hydroxyapatite matrix [19]. By contrast, materials like zirconia (Y-TZP) are about four times harder than natural enamel, which can cause wear and damage to opposing teeth during chewing [19].
Biomimetic materials aim to mimic this natural complexity. For example, bilayered composites and hybrid ceramics like PICN (polymer-infiltrated ceramic network) replicate the gradient hardness and elastic modulus found in natural teeth [3][19]. Enamel is roughly 95% hydroxyapatite by weight, while dentin consists of 75% hydroxyapatite and 20% organic matrix (primarily Type I collagen) [6]. Biomimetic materials are engineered to match these proportions and mechanical properties.
The way these materials bond to teeth also sets them apart. Conventional bonding methods can lead to collagen collapse and microleakage, often resulting in secondary decay. Biomimetic materials, however, form an "ion-exchange layer" or achieve "intrafibrillar mineralisation", creating a stronger, gap-free bond [3][19]. Some biomimetic resin composites even include microcapsules that release healing agents when cracks form, enabling self-repair – something conventional materials simply can’t do [3].
| Feature | Conventional Materials | Biomimetic Materials |
|---|---|---|
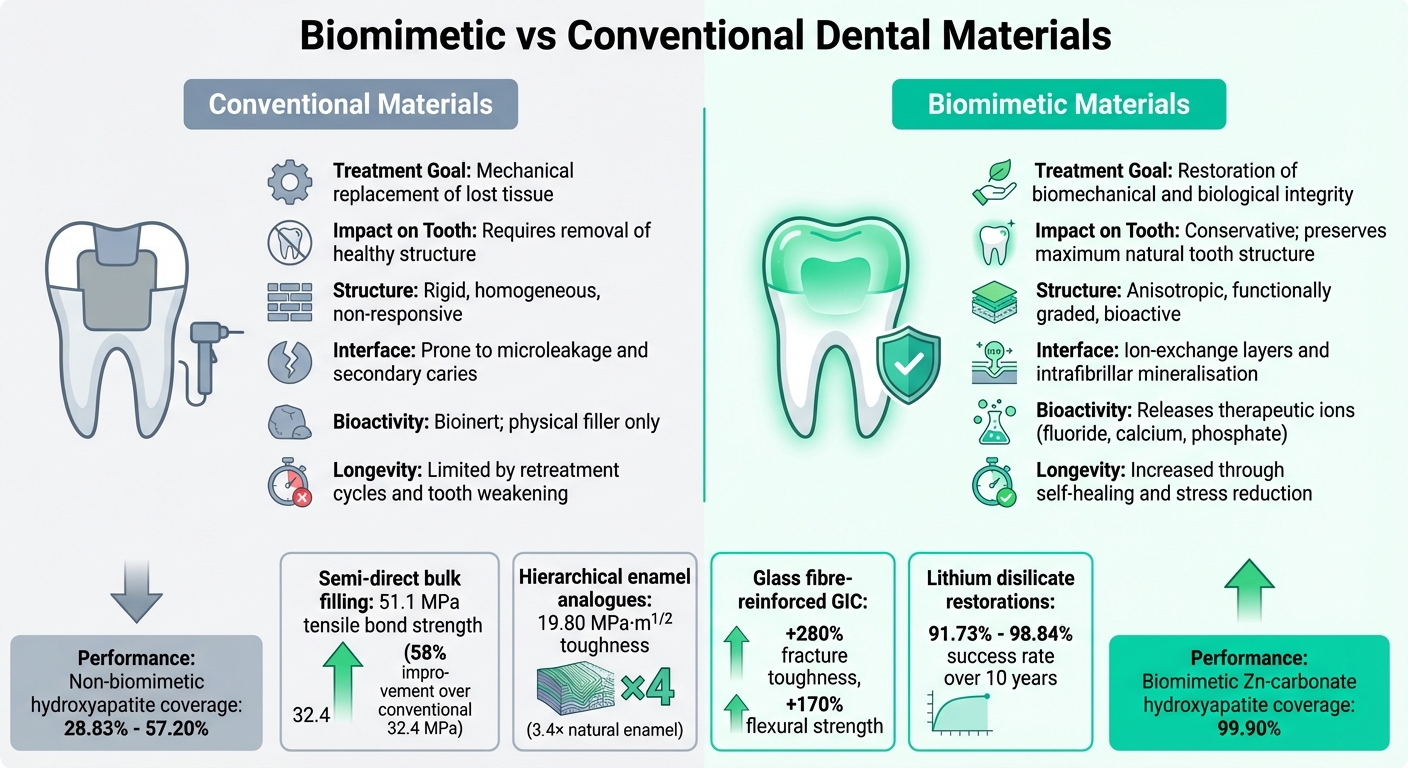
| Treatment Goal | Mechanical replacement of lost tissue | Restoration of biomechanical and biological integrity |
| Impact on Tooth Structure | Requires removal of healthy structure | Conservative; preserves maximum natural tooth structure |
| Structure | Rigid, homogeneous, and non-responsive | Anisotropic, functionally graded, and bioactive |
| Interface | Prone to microleakage and secondary caries | Ion-exchange layers and intrafibrillar mineralisation |
| Bioactivity | Bioinert; primarily acts as physical filler | Releases therapeutic ions (fluoride, calcium, phosphate) |
| Longevity | Limited by retreatment cycles and tooth weakening | Increased longevity through self-healing and stress reduction |
These differences in structure and function lead to clear performance benefits. For instance, biomimetic Zn-carbonate-substituted hydroxyapatite (microRepair®) achieved 99.90 ± 0.12% enamel coverage in lab studies, far surpassing commercial non-biomimetic hydroxyapatites, which ranged from 28.83% to 57.20% [6]. Similarly, adding 10 wt% hollow discontinuous glass fibres to Glass Ionomer Cements boosted fracture toughness by 280% and flexural strength by 170% [3]. These findings highlight the practical advantages of biomimetic materials in dental care.
Clinical Applications and Challenges
Applications in Restorative Dentistry
Advancements in biomimetic materials are making their way from the lab to the dental chair, offering a variety of solutions for restorative treatments. Nanocomposites, for instance, are now widely used in anterior restorations due to their excellent wear resistance and natural translucency, making them ideal for aesthetic applications [5]. Similarly, bioactive glasses are being incorporated into fillings and crown cementation, actively aiding in the remineralisation of carious dentine [5]. For issues like enamel erosion or hypersensitivity, coatings made from supramolecular protein matrices, such as elastin-like recombinamers, are proving effective. These coatings promote the growth of apatite nanocrystals, helping to reconstruct the intricate prismatic structure of natural enamel [1].
In endodontics, biomimetic approaches are pushing boundaries. Stem cell therapy and bioactive antimicrobials are now being used to restore pulp vitality, moving away from the traditional "remove and replace" philosophy [4]. Self-healing composites are another breakthrough, designed to release healing agents when cracks appear, significantly reducing failure rates [5]. Even everyday oral care products are benefiting from biomimetic innovations, with hydroxyapatite now a common ingredient in toothpastes and mouthwashes. This compound helps fill microscopic defects and prevents plaque formation [6].
A standout example of clinical success comes from a 2024 study conducted by the Medical University Sofia on lithium disilicate restorations. The study, led by Angela Gusiyska, tracked 86 lithium disilicate (e.Max Press) indirect restorations in 32 patients over a 10-year period. The results were impressive, showing a success rate of 91.73% to 98.84%. Only four restorations failed due to fractures by the 5-year mark, representing a failure rate of just 4.65%. Gusiyska summarised the findings:
"Lithium disilicate ceramic restorations provide a good treatment alternative for a 5- to 10-year period of observation, and they can be successfully applied in dental practice in 91.73% to 98.84% of cases" [21].
While these applications highlight significant progress, there are still challenges that need to be addressed for long-term reliability.
Challenges and Evidence Gaps
Despite these advancements, several hurdles remain. Reproducing the intricate three-level hierarchy of natural enamel – from nanowires to microbundles and macroarrays – is a major engineering challenge. Current materials often only replicate one or two of these levels, falling short of fully mimicking enamel’s complexity [2][19]. Experimental remineralisation techniques also face practical barriers, such as the use of toxic components or lengthy application times, with some treatments requiring up to 12 hours to be effective [1]. Even dental implants, while initially successful, see a significant drop in complication-free success rates after 5–10 years, often due to biomechanical stress or tissue degradation [20].
Another issue is the trade-off between stiffness and hardness versus the viscoelastic properties needed to absorb chewing forces. Striking this balance remains a significant obstacle in material design [2]. Furthermore, long-term in vivo studies are still limited, and there’s a lack of standardised manufacturing methods for complex hierarchical materials [19]. High costs associated with advanced fabrication techniques, such as 3D bioprinting, also pose a barrier to widespread adoption [4][19].
Ultimately, while laboratory results are promising, more robust clinical validation and long-term data are essential to fully understand how these materials perform over decades of use in real-world settings. These gaps highlight the need for continued research and innovation to translate these technologies into reliable, everyday dental solutions.
Conclusion
Biomimetic materials are changing the way dental professionals approach restorative care. Instead of merely filling cavities with inert materials, dentistry now embraces bioactive solutions that encourage healing and remineralisation. Advances like nanocomposites, which imitate the mechanical properties of natural enamel, and self-healing composites that repair micro-cracks, are broadening the scope of preserving natural tooth structures. These developments not only improve the performance of restorations but also influence the evolution of clinical practices.
To summarise, Hierarchical Enamel Analogues have shown a toughness of 19.80 MPa·m^(1/2) – 3.4 times greater than natural enamel [2]. Additionally, supramolecular protein matrices have been proven to rebuild mineralised layers up to 10 μm thick on eroded surfaces [1]. This dual focus on preservation and regeneration is at the heart of modern restorative dentistry.
However, there are still hurdles to overcome. While these breakthroughs mark a major step forward, challenges like clinical validation and standardising manufacturing processes remain. With oral health issues impacting nearly 50% of the global population and costing approximately US$544 billion annually [1], the potential influence of these innovations goes far beyond individual treatments. For Australian patients, staying informed about these advancements can lead to more meaningful conversations with dental professionals about treatment options that prioritise both immediate outcomes and the long-term health of their teeth.
FAQs
Am I a suitable candidate for biomimetic restorations?
When it comes to biomimetic restorations, whether you’re a good candidate depends on several factors, including your overall oral health and the current state of your teeth. These methods focus on preserving as much of your natural tooth structure as possible, making them a great option for addressing problems like early-stage decay, small fractures, or even cases where the tooth pulp is exposed.
Your dentist will evaluate your specific needs, taking into account things like your oral hygiene habits and the severity of the damage, to decide if this treatment is the right fit for you.
How long do biomimetic fillings and crowns usually last?
Biomimetic fillings typically last between 10 and 15 years, while crowns and ceramic restorations can endure for 20 years or more when maintained properly. Their lifespan largely depends on factors like maintaining good oral hygiene, scheduling regular dental check-ups, and steering clear of habits such as teeth grinding or chewing on hard objects.
Are biomimetic materials safe and supported by long-term evidence?
Biomimetic materials in dental surgery have gained recognition for their safety and increasing evidence of long-term success. Research has shown their effectiveness in areas like enamel and dentin repair, tissue regeneration, and enhancing implant surfaces. Consistent findings from studies underline their positive impact, solidifying their importance in restorative and regenerative dentistry.
Related Blog Posts
- Wear Resistance of Polymer-Based Restoratives
- Advances in Dental Adhesives: What to Know
- Bond Strength of CAD/CAM Materials with Adhesives
- Biomimetic Tooth Restoration: Key Benefits
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





