







Foreign Body Response in Dental Implants Explained
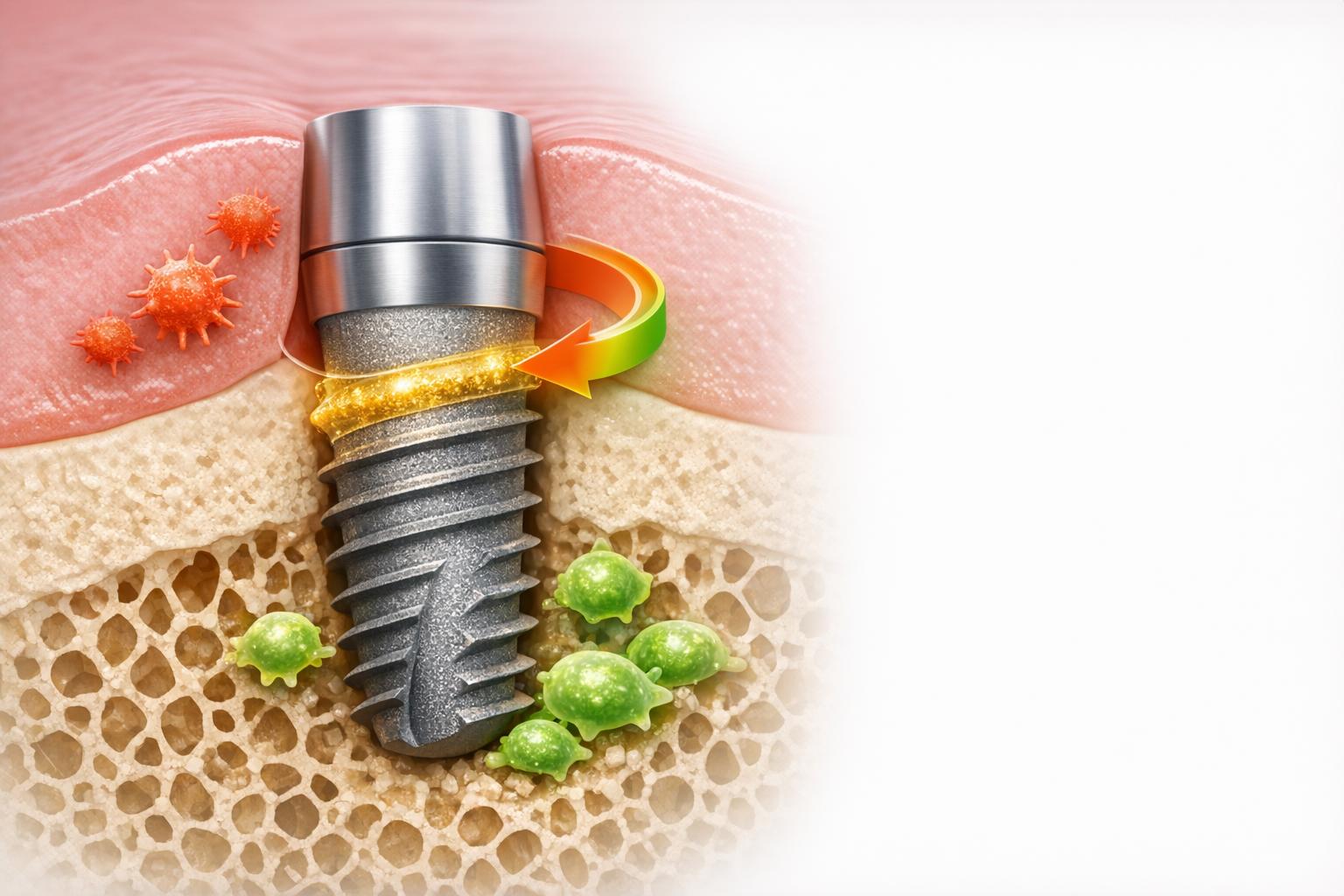
When a dental implant is placed, your immune system reacts to the material as foreign, triggering a process called the foreign body response (FBR). This response determines whether the implant integrates with your jawbone (osseointegration) or fails due to fibrous tissue formation. Here’s a quick breakdown:
- Initial Reaction: Blood proteins coat the implant, attracting immune cells like neutrophils and macrophages.
- Inflammation Phases: Acute inflammation (first two weeks) clears debris, followed by a chronic phase where macrophages decide the outcome.
- Key Outcome: Successful implants bond with bone (95% success rate in healthy people), while excessive inflammation leads to fibrous encapsulation and implant failure.
- Influencing Factors: Implant surface properties (like roughness and wettability), patient health (e.g., diabetes, smoking), and surgical precision all play major roles.
Foreign Body Reaction (FBR) – Comparison of a Material with a Low and a Strong FBR
Understanding how the body reacts to different materials is a key part of dental implants explained for patients considering the procedure.
sbb-itb-2be92ed
The Stages of Foreign Body Response in Dental Implants
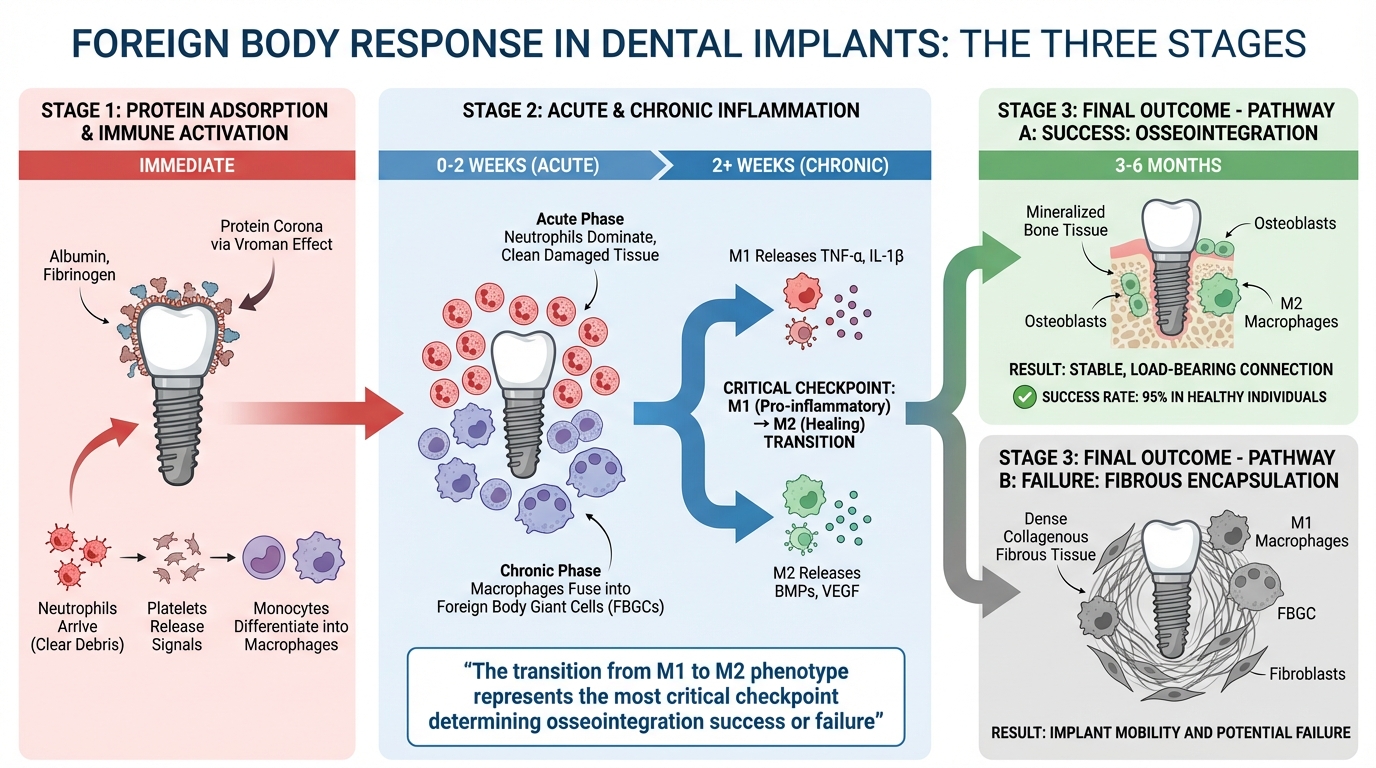
The Three Stages of Foreign Body Response in Dental Implants
Protein Adsorption and Immune Response Activation
When a dental implant process begins when the fixture is inserted into the jawbone, blood proteins immediately coat its surface, creating what’s called a "protein corona." This layer, formed by proteins like albumin and fibrinogen, adheres to the titanium surface through the Vroman effect [3][1]. This initial coating not only represents the first point of contact between the implant and the immune system but also plays a role in inflammatory cell adhesion via integrins. Neutrophils are the first responders, clearing surgical debris, while platelets release signals to attract monocytes, which then differentiate into macrophages [1]. This protein layer essentially sets the stage for the immune system’s response.
Acute and Chronic Inflammation
The immune response progresses through two main phases. During the acute phase, which starts immediately after implantation, neutrophils dominate the site, working to clean up damaged tissue and any contaminants [1][5]. This phase builds on the earlier protein-driven recruitment of immune cells. However, if inflammation persists, it transitions into a chronic phase. Here, macrophages may fuse to form Foreign Body Giant Cells (FBGCs), which can degrade the implant by releasing reactive oxygen species and acids [1][5]. The key to a successful outcome lies in how quickly macrophages switch from the pro-inflammatory M1 phenotype to the healing-focused M2 phenotype. As Xiao-Chong Jian from Hainan Medical University explains, "The transition from M1 to M2 phenotype represents the most critical checkpoint determining osseointegration success or failure" [5].
Fibrous Encapsulation or Osseointegration
The final stage of this immune response determines whether the implant integrates successfully or fails. In favourable outcomes, the immune system achieves a balance where bone tissue bonds directly to the implant, resulting in osseointegration within three to six months [3][5]. In this case, the implant becomes encased in living bone, creating a strong and stable connection. On the other hand, prolonged M1 activation can lead to the formation of a dense fibrous capsule by fibroblasts. This collagen barrier prevents direct bone attachment, resulting in implant instability [1][3].
| Outcome | Primary Cells | Tissue Formed | Clinical Result |
|---|---|---|---|
| Osseointegration | M2 Macrophages, Osteoblasts | Mineralised bone tissue | Stable, load-bearing connection |
| Fibrous Encapsulation | M1 Macrophages, FBGCs, Fibroblasts | Dense collagenous fibrous tissue | Implant mobility and potential failure |
These stages illustrate why dental implants have a success rate exceeding 95% in healthy individuals [5].
How Osseointegration Works as a Modified Foreign Body Reaction
Macrophage Polarisation and Implant Success
Osseointegration is essentially the body’s modified response to a foreign object, where the immune system isolates the implant by forming a protective bone layer around it, rather than fully integrating it as a natural part of the body. As Professor Tomas Albrektsson from the University of Gothenburg explains, "Osseointegration is a foreign body reaction where interfacial bone is formed as a defense reaction to shield off the implant from the tissues" [8][9].
The role of macrophages is central to this process and directly impacts the success of the implant. Initially, after the implant is placed, M1 macrophages dominate. These cells release inflammatory signals like TNF-α and IL-1β, which help to clear surgical debris and prepare the site. Within about two weeks, however, these M1 macrophages transition into M2 macrophages, which release healing factors such as BMPs and VEGF. These factors recruit bone-forming cells, setting the stage for bone regeneration [5][10]. This shift from inflammation to healing acts as a "biological switch." While controlled inflammation is essential for bone regeneration, prolonged inflammation can lead to complications.
Advanced implant surfaces, such as SLActive®, have been shown to enhance this process significantly. These surfaces increase the recruitment of M2 macrophages by approximately 92% compared to standard surfaces, which helps speed up the healing process [5]. Ultimately, this macrophage-driven mechanism determines whether bone formation or fibrous tissue encapsulation will dominate around the implant.
Bone Formation Versus Fibrous Encapsulation
Once macrophage activity sets the stage, the subsequent tissue response decides the fate of the implant. Successful osseointegration achieves what’s known as Foreign Body Equilibrium (FBE), where mineralised bone forms a stable, load-bearing interface with the implant [8][5]. This bone capsule can remain functional for decades – some cases have been documented to last over 50 years [8][9].
However, if the M1 phase lingers too long or if M2 macrophages inadvertently trigger fibrosis, the outcome can shift. In such cases, factors like TGF-β and Galactin-3 may signal fibroblasts to produce dense collagen fibres instead of bone. This results in a soft-tissue capsule rather than a solid bone attachment, leading to implant mobility and eventual failure.
The key to these differing outcomes lies in the RANK-RANKL-OPG signalling axis. M1 macrophages promote bone resorption through RANKL, while M2 macrophages support osteoblast activity and bone formation [5][10]. Therefore, understanding and carefully managing these immune responses is critical for improving the longevity of dental implants and achieving better clinical results.
Factors That Affect Foreign Body Response in Dental Implants
Implant Surface Properties and Material Choices
The relationship between implant surface properties and the body’s immune response is a critical factor in dental implant success. A key aspect is how these surfaces influence protein adsorption and the subsequent biological reactions.
Surface roughness is particularly important. For example, micro-rough surfaces like those created through sandblasting and acid-etching (SLA) techniques significantly increase the surface area – from approximately 0.078 µm on machined surfaces to about 1.55 µm on SLA-treated surfaces. This expanded surface area enhances both mechanical anchorage and protein adsorption, aiding the healing process [11]. However, overly rough surfaces can release wear particles, which may activate the NLRP3 inflammasome, leading to chronic inflammation [5].
Surface wettability, or how well a surface interacts with water and proteins, also plays a pivotal role. Traditional SLA surfaces are hydrophobic, with a water contact angle of around 114.6°. This hydrophobicity can hinder initial protein binding and cellular attachment [11]. On the other hand, hydrophilic surfaces, such as those with SLActive properties, improve protein adsorption and help modulate the immune response for better healing outcomes. Some advanced surfaces, like anatase-coated SLA, achieve near-superhydrophilic conditions with water contact angles as low as 3.8°, which has been linked to faster early bone healing [11].
Modern implant designs are moving beyond inert materials to actively modulate the immune response. For instance, titanium nanotube arrays with diameters around 30 nm encourage the polarisation of pro-healing M2 macrophages, while larger structures may lean toward an inflammatory M1 response [5]. Additionally, bioactive coatings, such as those incorporating zinc or zinc combined with BMP-2, enhance M2 macrophage recruitment and improve bone-implant contact compared to uncoated surfaces [5]. These innovations play a crucial role in steering the body towards osseointegration rather than fibrous encapsulation.
While implant surface properties set the stage for biological responses, patient-specific factors heavily influence the overall healing process.
Patient-Specific Factors
An individual’s health and lifestyle significantly impact the integration of dental implants. Systemic conditions such as type 2 diabetes, hypertension, and thyroid disorders can disrupt the resolution of inflammation, potentially shifting the healing process from bone formation to fibrous encapsulation. This risk increases with age, as "inflammaging" – a chronic low-grade inflammatory state – becomes more pronounced [3].
Lifestyle choices, like smoking and oral hygiene practices, also play a major role. Smoking pushes the immune system toward a pro-inflammatory M1 state, while poor oral hygiene and plaque buildup continuously stimulate immune responses, disrupting the balance required for successful osseointegration [3][6]. These challenges highlight the importance of thorough pre-surgical evaluations and strict post-operative care. Addressing systemic and behavioural risk factors is vital, as they can substantially reduce the likelihood of implant success [3][5].
Together, these material and patient-specific factors set the stage for the clinical outcomes discussed in the next section.
Clinical Effects of Fibrous Encapsulation
Link Between Fibrous Encapsulation and Peri-Implantitis
When the body fails to achieve proper osseointegration, it can lead to fibrous encapsulation – a condition where a layer of collagen forms between the implant and the bone instead of direct bone-to-implant contact [3]. This soft tissue barrier lacks the mechanical stability needed for implant success, often resulting in mobility and eventual prosthetic failure. Unlike the reparative M2 macrophage activity seen in successful osseointegration, fibrous encapsulation is marked by a chronic inflammatory state driven by pro-inflammatory M1 macrophages and foreign body giant cells [2].
"The inability to resolve the initial inflammatory response leads to a chronic inflammatory state and fibrous encapsulation of the implant, which is characteristic of a foreign body response that leads to early implant failure." – PubMed/Periodontology 2000 [2]
This unrelenting inflammation can increase the risk of peri-implantitis. While plaque is the main cause of peri-implant disease, an imbalanced immune response can speed up bone loss. Additionally, titanium wear particles released from the implant surface can activate the NLRP3 inflammasome, worsening inflammatory bone loss and causing localised infections. In severe cases, this may require surgical removal of the implant [5]. These challenges highlight the importance of targeted intervention to manage the foreign body response effectively.
How to Reduce Fibrous Encapsulation Risk
Reducing the risk of fibrous encapsulation involves a combination of precise surgical techniques and material innovations. Surgical accuracy is crucial. Using imaging-guided systems instead of manual methods can minimise tissue trauma and reduce the risk of blood vessel injury during implant placement [3]. Flapless vs. flapped implant techniques have also been shown to lower matrix metalloproteinase-8 levels and limit marginal bone loss compared to traditional approaches [5].
Material advancements play a significant role in modulating the immune response. Hydrophilic implant surfaces encourage better protein adsorption and reduce pro-inflammatory cytokine activity, directly lowering the likelihood of fibrous encapsulation [5]. Coatings that incorporate bioactive ions, such as strontium or zinc, enhance bone-implant contact [5]. Additionally, nanotube arrays can promote the M2 macrophage response, which is essential for successful osseointegration [5].
Patient-specific factors must also be addressed. Managing systemic conditions like type 2 diabetes, promoting smoking cessation, and maintaining strict oral hygiene can help reduce the pro-inflammatory environment that contributes to fibrous encapsulation [3][5]. Ensuring stable implant-abutment connections is equally important, as this prevents micromotion and the release of titanium particles that could trigger inflammation [5]. By focusing on surgical precision, material design, and patient care, clinicians can guide the foreign body response towards successful osseointegration.
Conclusion
Osseointegration is not a static event but an active, immune-driven process where the body surrounds the implant with bone rather than fibrous tissue [7]. This delicate balance, often referred to as "foreign body equilibrium", is crucial for the implant’s success over its lifetime. Disruptions – whether from plaque build-up, mechanical injury, or titanium particle release – can tip the immune response from bone preservation to bone loss [7]. This highlights the importance of careful clinical management.
A key part of this process is the shift from M1 to M2 macrophages, which supports bone formation directly on the implant surface [5]. When this transition falters, chronic inflammation can occur, leading to fibrous encapsulation – a soft tissue layer that jeopardises implant stability. Research even shows that removing macrophages entirely can eliminate the foreign body response altogether, underscoring their vital regulatory role [4].
Clinicians can actively shape these immune responses through thoughtful choices in materials, surgical approaches, and patient care. For instance, hydrophilic implant surfaces with bioactive ion coatings encourage M2 macrophage activity, while minimally invasive techniques help curb the initial inflammatory response [5]. Additionally, addressing patient-specific factors like managing type 2 diabetes, promoting smoking cessation, and maintaining excellent oral hygiene plays a pivotal role in preserving this immune balance [3][5].
"The long-term clinical function is dependent on a foreign body equilibrium, that if disturbed may lead to impaired clinical function of the implant… resulting in the start of bone resorption." – Ricardo Trindade, PhD Student, Malmö University [7]
Acting early to counter peri-implant bone loss is essential to restoring balance and preventing implant failure. By viewing osseointegration as an ongoing immune process, dental professionals can better support healing and maintain success rates exceeding 95% in healthy patients [5].
FAQs
How can I tell if my implant is osseointegrating properly?
To determine if osseointegration has occurred, focus on two key indicators: stability and the absence of pain. Osseointegration happens when the bone successfully bonds with the implant, a process that usually takes a few months. A properly integrated implant should remain firmly in place without any movement or discomfort. However, if you notice ongoing pain or the implant feels unstable, it’s important to see your dentist for a thorough assessment.
What early signs might suggest fibrous encapsulation or implant failure?
Early indicators of fibrous encapsulation or implant failure can manifest as inflammation, swelling, or discomfort in the area surrounding the implant. Sometimes, there may be visible signs of the implant loosening or shifting, which could point to a foreign body reaction or issues with the implant’s integration into the bone.
What can I do before and after surgery to reduce chronic inflammation around an implant?
To keep chronic inflammation at bay around a dental implant, it’s crucial to maintain excellent oral hygiene and stick to your dentist’s aftercare advice. Focus on controlling plaque buildup, schedule regular professional cleanings, and follow a soft food diet during the healing phase. Stay away from irritants, use gentle oral care techniques, and manage any discomfort with prescribed medications. These steps can help promote healing and lower the chances of inflammation.
Related Blog Posts
- Osteoimmunology in Implant Healing
- How Hybrid Coatings Improve Osseointegration
- Surface Modifications for Better Osseointegration
- How Surface Modifications Improve Implant Biocompatibility
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





