







When to Consider DBS for Facial Pain

Living with chronic facial pain can feel unbearable, especially when standard treatments fail. For severe cases that don’t respond to medications, nerve blocks, or other therapies, Deep Brain Stimulation (DBS) may be an option. DBS is a surgical procedure that uses electrical pulses to interrupt pain signals in the brain, offering relief for treatment-resistant conditions like trigeminal neuralgia, persistent idiopathic facial pain, or postherpetic neuralgia.
Key Points:
- DBS is a last-resort treatment for chronic facial pain when all other methods have been exhausted.
- It involves implanting electrodes in the brain to regulate abnormal pain signals.
- Candidates often endure years of pain before qualifying for DBS, with patients experiencing an average of 50% pain reduction after the procedure.
- Risks include surgical complications, device-related issues, and side effects like tingling or unusual sensations, but these are often manageable with adjustments.
DBS isn’t for everyone. A thorough evaluation by a multidisciplinary team is essential to determine eligibility and ensure the best possible outcome. If you’ve tried everything else without relief, it might be time to explore DBS as a potential option.
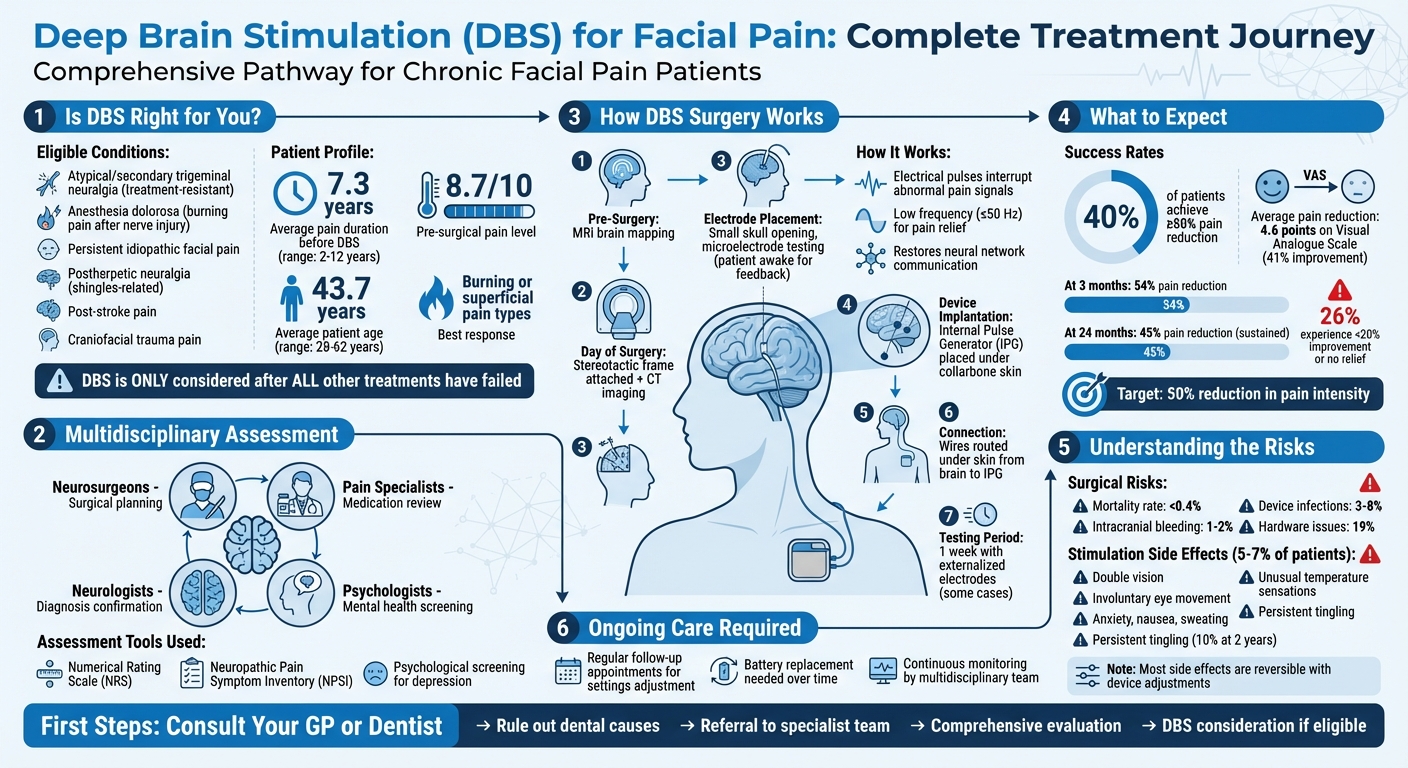
DBS Treatment Journey: From Evaluation to Pain Relief for Chronic Facial Pain
Treatment Options for Orofacial Pain
Standard Treatments
When addressing orofacial pain, clinicians typically start with conservative, well-researched methods. Medications like anticonvulsants (e.g., carbamazepine, gabapentin, pregabalin) and antidepressants (e.g., amitriptyline, duloxetine) are often prescribed to regulate nerve signalling.
For odontogenic pain, the focus is on reducing inflammation through procedures such as pulpotomy or root canal therapy. Interestingly, research suggests that pulpotomy can provide similar immediate pain relief to a full pulpectomy for cases of symptomatic irreversible pulpitis [4]. Non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen are commonly used, and combining 600 mg of ibuprofen with paracetamol has been shown to offer effective relief from both pain and inflammation. Opioids, such as codeine, are generally avoided due to their central acting properties and associated risks.
"Multidisciplinary treatment is the gold standard", explains E Russell Vickers, a Pain Medicine Specialist.
This multidisciplinary approach often integrates medication with psychological and behavioural therapies. For temporomandibular disorders (TMD), self-management plays a key role. Techniques like jaw rest, applying heat or ice, facial massage, and making dietary adjustments form the backbone of care. In more acute situations, nerve blocks or supplemental anaesthetic techniques may be used to manage pain or facilitate dental procedures.
However, if these standard methods fail to provide adequate relief, more advanced treatments may need to be considered.
When Standard Treatments Don’t Work
Despite following standard protocols, some patients continue to experience severe, persistent pain. For instance, around 25% of those treated for symptomatic irreversible pulpitis may return within a week due to unresolved pain [4]. Additionally, conditions like central sensitisation – where the central nervous system becomes overly reactive – can lead to ongoing, spontaneous pain even after the initial injury has healed.
In cases where treatments like peripheral nerve blocks or dental procedures fail, or when new pain arises post-treatment (as seen in conditions like Anesthesia Dolorosa), it may indicate that the pain mechanisms have progressed beyond the peripheral nerves. Alarmingly, untreated pain increases the likelihood of developing chronic pain by 19% with each passing day [4]. Such scenarios might warrant exploring neuromodulation therapies, including deep brain stimulation, or high-frequency stimulation, but these are typically considered only after exhausting less-invasive options.
sbb-itb-2be92ed
Who Can Receive DBS Treatment?
Medical Assessment and Diagnosis
Deep Brain Stimulation (DBS) is typically reserved for individuals dealing with chronic, treatment-resistant facial pain. It’s not a first-line treatment – specialists only consider it after all other options have been exhausted. The evaluation process involves a team of experts, including neurosurgeons, pain specialists, and psychologists, who work together to determine if DBS is the right course of action [2][3].
"DBS is only considered when medications, nerve procedures, and other surgeries have failed to bring relief." – Pacific Neuroscience Institute [3]
Patients go through rigorous pain assessments, using tools like the Numerical Rating Scale (NRS) and the Neuropathic Pain Symptom Inventory (NPSI). Research shows that pre-surgical pain levels average 8.7 out of 10 on the NRS [2]. On average, candidates have endured pain for 7.3 years before qualifying for DBS, with cases ranging from 2 to 12 years [2]. Specialists also pay close attention to the nature of the pain – burning or superficial pain often responds more favourably to certain DBS targets compared to deep, pressing sensations [2].
A critical part of the assessment is psychological screening. This step helps rule out major depression or other psychiatric conditions that could complicate the treatment process [2]. By identifying patients who are both physically and mentally prepared for the procedure, the team maximises the likelihood of a positive outcome while minimising risks.
This comprehensive evaluation ensures that only the most suitable candidates are considered for DBS.
Factors That Affect Eligibility
DBS candidates often include individuals with specific conditions such as:
- Atypical or secondary trigeminal neuralgia that doesn’t respond to standard treatments.
- Anesthesia dolorosa, a burning pain following nerve injury or previous trigeminal neuralgia surgery.
- Persistent idiopathic facial pain, which is constant pain without an identifiable structural cause.
- Postherpetic neuralgia, stemming from shingles that affect the trigeminal nerve.
- Pain caused by stroke or craniofacial trauma [2][3].
Age and general health also play a role in determining eligibility, though there’s no strict age limit. Clinical studies show candidates range in age from 28 to 62 years, with an average age of 43.7 years [2]. Beyond age, overall health is crucial – patients must be in reasonably good condition without chronic illnesses that could increase surgical risks.
The goal of DBS is a 50% reduction in pain intensity, but it’s important to note that not every patient will achieve this. Around 26% may experience less than a 20% improvement or no relief at all [2]. This highlights the importance of the detailed evaluation process, ensuring DBS is only pursued when all other treatments for intractable orofacial pain have failed.
Brain Stimulation for Face Pain-Mayo Clinic
How DBS Relieves Facial Pain
Deep brain stimulation (DBS) offers a meticulously planned neurosurgical option for individuals whose severe orofacial pain has resisted all other general dental treatments. To understand its effectiveness, it’s important to look at both the surgical process and the way DBS works to alleviate pain.
The DBS Surgery
The DBS procedure involves a series of carefully orchestrated steps. It begins with an MRI scan to map the brain. On the day of surgery, a stereotactic frame is attached to the patient, and CT imaging is used to confirm the precise path for electrode placement [7]. Surgeons then make an incision in the scalp and drill a small opening in the skull. Using a microelectrode, they record brain signals and test stimulation before implanting the permanent electrode [7].
For orofacial pain, the main target is the Ventral Posterior Medial (VPM) nucleus of the thalamus, which processes sensory input from the face and head [6]. Other frequently targeted areas include the periaqueductal grey (PAG), periventricular grey (PVG), and the anterior cingulate cortex (ACC) [2][3]. During the surgery, patients are often kept awake for part of the procedure to provide feedback – such as reporting sensations of tingling or warmth – which helps confirm the correct placement of the electrodes [6].
Once the electrodes are implanted, a battery-powered device called the Internal Pulse Generator (IPG) is placed under the skin, usually near the collarbone. Thin wires are routed under the skin from the electrodes in the brain to the IPG [7]. In some cases, the electrodes are externalised for about a week to test their effectiveness before the permanent pulse generator is implanted [6].
This detailed process ensures the groundwork is laid for DBS to effectively modulate pain signals.
How the Stimulation Works
When activated, DBS sends electrical pulses to the brain that interrupt abnormal pain signals [3]. But it doesn’t just block pain – it appears to reset neural communication to a more balanced state.
Victor Mandat from the Department of Neurosurgery at the Maria Sklodowska-Curie National Research Institute of Oncology explains, "The leading theories indicate that electrical stimulation introduced by DBS restores neural network communication to a more physiological state" [2].
The success of DBS depends heavily on the stimulation settings. Lower frequencies (≤50 Hz) are generally used for pain relief, while higher frequencies (>70 Hz) can potentially increase pain [6]. The electrical pulses influence axons near the electrodes, opening and closing voltage-gated sodium channels, which helps regulate the transmission of pain signals [2].
Different areas of the brain contribute to pain relief in unique ways. For instance, stimulating the PAG or PVG may inhibit pain responses and trigger the release of natural opioids, while targeting the thalamus can replace pain with a pleasant tingling sensation (paraesthesia) [2][6]. Focusing on the anterior cingulate cortex can also help address the emotional distress caused by chronic pain. For those seeking advanced care, specialist dental treatments can also play a role in managing complex oral health issues.
Research supports these benefits. In one study involving patients with neuropathic facial pain, the Numeric Pain Rating Scale (NRS) showed a 54% reduction in pain at the three-month mark, and this improvement remained at 45% after 24 months. Burning or superficial pain showed an even greater improvement of 53% [2].
Results and Risks of DBS
Pain Relief and Success Rates
Deep brain stimulation (DBS) shows mixed outcomes for individuals dealing with chronic facial pain. Research, including a meta-analysis, indicates that DBS can reduce pain by an average of 4.6 points on the Visual Analogue Scale within three months – a reduction of about 41%. Around 40% of patients with chronic refractory facial pain experience at least a 50% pain reduction [5]. Interestingly, the success of DBS doesn’t seem to depend much on factors like age, how long the pain has lasted, or the specific area of the brain targeted [5].
For example, in a study focusing on post-stroke neuropathic pain, 7 out of 12 participants were able to stop using pain medications entirely after undergoing DBS [8]. However, the results are not consistent across all patients, and individual experiences vary [3]. Over time, some patients may notice that the benefits decrease, though adjusting device settings often helps restore relief [8].
Possible Risks and Complications
While DBS offers potential relief, it also comes with risks inherent to brain surgery. About 19% of patients experience hardware-related issues, such as infections or lead fractures [5]. Surgical risks include intracranial bleeding, infections, and thromboembolic events [3][2]. Additionally, approximately 5–7% of patients experience side effects related to stimulation, which can include double vision, involuntary eye movement, anxiety, nausea, sweating, or unusual sensations of warmth or cold [2][5]. Some individuals may also feel persistent pins and needles or tingling sensations, even when the device is turned off [2].
The good news is that most stimulation-related side effects are reversible. Adjustments to parameters like amplitude, frequency, or pulse width during follow-up appointments can often resolve these issues [3][2].
DBS requires ongoing commitment. Regular follow-ups are crucial for fine-tuning the settings [3], and the battery-powered pulse generator will eventually need maintenance or replacement [3][8]. Patients should approach DBS as a long-term treatment rather than a one-time solution.
The Need for Team-Based Care
Pain Specialists and Neurologists
Chronic orofacial pain is a complex condition that doesn’t fall neatly into one medical specialty, which can leave patients without proper care. Effective treatment often requires collaboration between medical and dental professionals.
When considering treatments like Deep Brain Stimulation (DBS), a multidisciplinary approach becomes critical. Pain specialists focus on managing medication protocols, including antiepileptic drugs and mood-stabilising treatments, and determine when conservative methods have been fully explored[2]. Neurologists and neurosurgeons work together to pinpoint the root cause of the pain, whether it’s post-stroke pain, trigeminal neuralgia, or another neuropathic issue[3]. Psychologists also play a key role by evaluating patients for untreated conditions like major depression and providing support throughout the surgical journey[2].
"At Pacific Neuroscience Institute, our neurosurgical team carefully evaluates each patient to determine whether DBS is appropriate, working closely with pain specialists and neurologists to ensure a comprehensive approach."
– Pacific Neuroscience Institute[3]
This team-based care doesn’t end with the DBS procedure. Specialists continue to monitor outcomes, adjust stimulation settings, and address any complications that may arise. This ongoing collaboration ensures the best possible pain management while also allowing for seamless referrals and thorough evaluations of all potential causes of facial pain before moving to advanced treatments like DBS.
Support from Dental Practices
Dental practices play an equally important role in the early stages of care. As the first point of contact for many, dental professionals often perform initial assessments. In fact, 92% of patients with orofacial pain report consulting a health practitioner, with dentists being the most common choice[1]. Clinics like Complete Smiles Bella Vista are equipped to identify common causes such as toothaches, temporomandibular disorders (TMD), or other dental-related problems. When standard treatments fail to provide relief, these practices refer patients to specialised pain teams, neurologists, or neurosurgeons for further evaluation and potential advanced interventions like DBS.
This collaborative process ensures patients receive a thorough and well-rounded treatment plan rather than temporary solutions. Starting with a detailed dental assessment not only helps rule out simpler causes but also allows patients to transition more quickly to the specialised care they may need, avoiding unnecessary delays and procedures[1].
Conclusion: Is DBS Right for You?
Deep Brain Stimulation (DBS) is often considered a last-resort option for managing facial pain when medications, nerve procedures, or surgeries have failed to provide relief [3]. It has shown promise for conditions like Anesthesia Dolorosa, atypical Trigeminal Neuralgia, Postherpetic Neuralgia, and Persistent Idiopathic Facial Pain. These treatments tend to work best for pain that feels burning and superficial rather than deep and pressing [2].
Before undergoing DBS, a thorough evaluation by a multidisciplinary team – including neurosurgeons, pain specialists, neurologists, and psychologists – is a must. This process ensures that all other treatments have been tried and that your specific pain profile makes you a suitable candidate. In studies of neuromodulation, success is often defined as at least a 50% reduction in pain. On average, pain scores have been found to drop by 54% three months after DBS and by 45% after 24 months [2].
"DBS is only considered when medications, nerve procedures, and other surgeries have failed to bring relief."
– Pacific Neuroscience Institute [3]
It’s important to maintain realistic expectations. Around 10% of patients may experience increased paraesthesia or dysaesthesia even two years after the procedure [2]. Additionally, DBS carries surgical risks, including a mortality rate of less than 0.4%, intracranial bleeding in 1–2% of cases, and device-related infections in 3–8% of patients [2]. Regular follow-ups are necessary to fine-tune the stimulation settings and ensure ongoing effectiveness [3].
Weighing the potential benefits against these risks is essential. For those whose chronic facial pain has resisted all standard treatments, the first step is consulting a GP or dentist. They can help rule out dental causes and, if needed, refer you to specialists who can assess whether DBS might be the right option for you.
FAQs
How do I know my facial pain is “treatment‑resistant” enough for DBS?
Facial pain is often deemed treatment-resistant for deep brain stimulation (DBS) when it continues unabated despite attempts with both medication and behavioural therapies. DBS is generally considered for individuals experiencing persistent, refractory pain who have not achieved relief through conventional treatments and have undergone thorough evaluation to determine if they are suitable candidates.
What tests and assessments are done before being approved for DBS?
Before moving forward with DBS, patients go through a detailed evaluation process. This includes checking whether their condition is likely to improve with DBS, assessing their ability to handle both the surgery and the stimulation, and conducting a neuropsychiatric evaluation to review their mood and cognitive health. Additionally, specialised imaging, such as an MRI, is performed to map out the procedure. These steps are designed to ensure the treatment is both appropriate and safe for each individual.
What does DBS aftercare involve long term (programming and battery changes)?
Deep Brain Stimulation (DBS) requires ongoing care to ensure it continues to work effectively. This includes routine adjustments to the device’s programming, performed by healthcare professionals, to fine-tune its performance. Battery upkeep is another essential part of aftercare – this might mean recharging the device if it has a rechargeable battery or replacing it entirely if the battery is non-rechargeable. These measures are crucial for keeping the device functioning as intended over the long term.
Related Blog Posts
- Neurostimulation: Future of Dental Pain Relief
- High-Frequency Stimulation for Neuropathic Orofacial Pain
- Emerging Therapies in Orofacial Pain Management
- Trigeminal Neuralgia: Pain Relief Options
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





