







Trigeminal Neuralgia: Pain Relief Options

Trigeminal neuralgia (TN) is an extremely painful condition affecting facial nerves, often triggered by everyday activities like eating or talking. It can feel like sudden electric shocks and usually impacts one side of the face. Treatments range from medications like carbamazepine, to minimally invasive procedures, and even surgery for severe cases. Accurate diagnosis is crucial, as TN is often misdiagnosed as dental or sinus issues.
Key Takeaways:
- Symptoms: Intense, sudden facial pain triggered by simple actions.
- Causes: Often due to nerve compression or underlying conditions like multiple sclerosis.
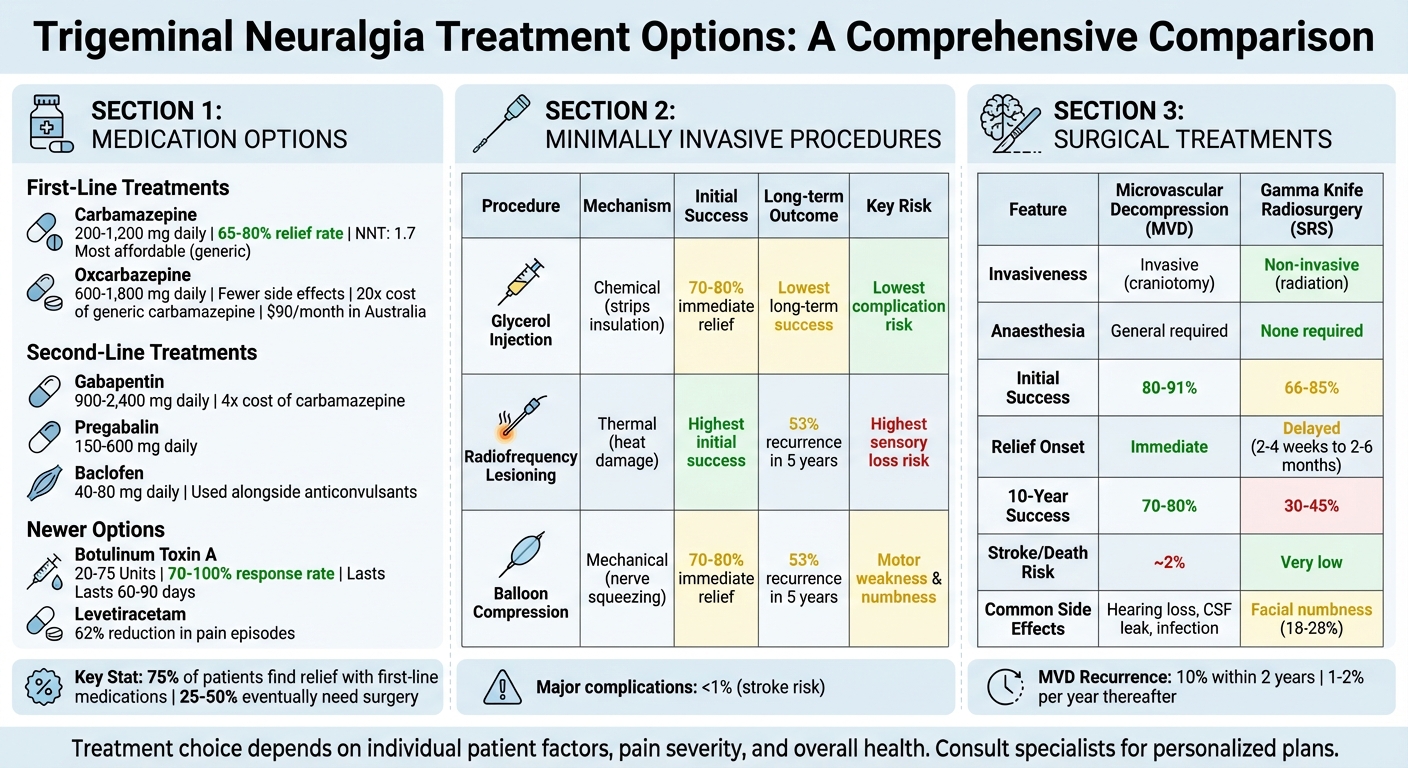
- Medications: First-line options include carbamazepine and oxcarbazepine, with alternatives like gabapentin or pregabalin for those who don’t respond.
- Procedures: Options like glycerol injections, radiofrequency lesioning, or balloon compression offer relief but may require repeat treatments.
- Surgery: Microvascular decompression provides long-term relief for many, while Gamma Knife radiosurgery is less invasive but less durable.
- Lifestyle Tips: Avoid triggers, reduce stress, and consider psychological support to manage the condition.
If you’re experiencing persistent facial pain that doesn’t respond to standard painkillers, see a GP early for proper diagnosis and treatment.
Trigeminal Neuralgia Treatment Options Comparison: Medications, Procedures, and Surgery
#100 How to treat TRIGEMINAL NEURALGIA with medications, surgery and interventional procedures
Medication Options for Pain Relief
Around 75% of patients find relief with first-line anticonvulsants, which work by slowing nerve impulses and easing pain [9][2]. These medications are part of a structured approach to managing trigeminal neuralgia (TN) after a proper diagnosis. Below is an overview of the primary and alternative medication options.
Carbamazepine and Oxcarbazepine
Carbamazepine is the go-to treatment and the only FDA-approved medication for TN. It stabilises nerve membranes by blocking voltage-sensitive sodium channels [8][9]. Dosages typically range from 200 to 1,200 mg daily, with 65 to 80% of patients experiencing relief within a week [8]. The Number Needed to Treat (NNT) for 50% pain relief is 1.7 [8].
"So predictable and powerful is the relief that if the patient does not respond at least partially to carbamazepine, reconsider the diagnosis of idiopathic trigeminal neuralgia." – Manish K Singh, MD, Chief of Neurology [9]
Despite its effectiveness, carbamazepine requires careful monitoring due to possible side effects like sedation, dizziness, nausea, and diplopia [8][10]. More severe risks include bone marrow suppression, hyponatraemia (low sodium levels), and, in rare cases, Stevens-Johnson syndrome, a serious skin reaction [8][10]. Routine blood tests are essential to monitor blood counts, liver function, and sodium levels [8][10]. Generic carbamazepine is also the most affordable option [9].
Oxcarbazepine is a first-line alternative for those who cannot tolerate carbamazepine. It works through a similar sodium channel blockade and is prescribed at 600 to 1,800 mg daily [10]. It tends to cause fewer side effects and has fewer drug interactions [10]. Common side effects include dizziness, drowsiness, and fatigue [8][10]. However, oxcarbazepine can be much pricier – up to 20 times the cost of generic carbamazepine [9]. In Australia, it costs about $90 per month and is not covered by the PBS for TN [8].
Gabapentin, Pregabalin, and Baclofen
When first-line treatments fail or cause intolerable side effects, second-line options come into play. Gabapentin (900 to 2,400 mg daily) and pregabalin (150 to 600 mg daily) target the alpha-2-delta subunit of voltage-gated calcium channels, offering an alternative mechanism for pain relief [8][9]. These medications are easier to adjust and have no known drug interactions, making them ideal for older patients or those on multiple medications [9][10]. Studies have shown gabapentin to provide complete relief in most cases of multiple sclerosis-related TN [9].
Gabapentin’s side effects include fatigue, drowsiness, ataxia, and confusion, while pregabalin may cause dizziness, weight gain, and blurred vision [8][10]. Gabapentin costs about four times more than generic carbamazepine [9].
Baclofen, a GABA-b receptor agonist, is often used alongside anticonvulsants rather than as a standalone treatment. Dosed at 40 to 80 mg daily, it works differently to inhibit sharp, stabbing pains [8][9][10]. Side effects include drowsiness, weakness, nausea, and low blood pressure [10]. Baclofen must not be stopped suddenly, as this can lead to seizures or hallucinations [10].
Newer Medication Approaches
For patients who don’t respond to first- or second-line treatments, newer options may help. Topiramate (100 to 400 mg daily) and levetiracetam (1,000 to 4,000 mg daily) offer alternative mechanisms by targeting sodium and calcium channels or synaptic vesicle proteins, respectively [10][8]. A meta-analysis of 354 patients suggested topiramate’s effectiveness is comparable to carbamazepine, though the evidence quality was limited [10]. Levetiracetam has shown promise as an add-on therapy, with one study reporting a 62% reduction in daily pain episodes [10].
Botulinum toxin A injections are another promising option for those who don’t respond to oral medications. Injected into trigger zones at doses of 20 to 75 Units, these treatments have shown a 70 to 100% response rate, with pain intensity and frequency dropping by 60 to 100% within four weeks [10]. The effects generally last 60 to 90 days [8][9]. This works by blocking the release of pain-related neuropeptides like substance P and glutamate [10].
Between 25% and 50% of patients eventually find medication ineffective and may require surgical alternatives [9]. Dosages for most drugs must be adjusted gradually to improve tolerance and prevent withdrawal or sudden pain flares [2]. Since TN can sometimes go into remission, patients might attempt to taper off medications after 6 to 12 months of being pain-free [9][2].
Minimally Invasive Procedures
When oral medications fall short or cause intolerable side effects, minimally invasive procedures offer a practical next step. These percutaneous treatments act as a bridge between medication and major surgery. Designed as outpatient options, they directly target the nerve, avoiding large incisions and providing a less invasive alternative to traditional surgical methods [12]. Below are some of the most common techniques used to disrupt pain signals effectively.
Glycerol Injections, Radiofrequency Lesioning, and Balloon Compression
Glycerol rhizotomy involves inserting a needle through the cheek into the trigeminal cistern, where a sterile liquid glycerol is injected. This strips the nerve’s insulation, blocking pain signals [11][4]. While this method has the lowest risk of complications, its long-term success rates are also the lowest [6].
Radiofrequency lesioning uses a current delivered through an electrode to heat and damage a specific part of the nerve [11]. This method offers a higher initial success rate compared to glycerol injections but comes with a greater risk of permanent sensory loss [6].
Balloon compression involves inflating a small balloon at the base of the skull for about one minute. This compresses the nerve, disrupting its ability to transmit pain signals [11].
These procedures provide immediate pain relief for 70%–80% of patients [12]. However, pain often recurs within five years for about 53% of patients, necessitating repeat treatments [5]. Here’s a quick comparison of these techniques:
| Procedure | Mechanism | Benefit | Risk |
|---|---|---|---|
| Glycerol Injection | Chemical (strips insulation) | Lowest risk of complications [6] | Lower long-term success rates [6] |
| Radiofrequency | Thermal (heat damage) | Higher initial success rates [6] | Highest risk of sensory loss [6] |
| Balloon Compression | Mechanical (nerve squeezing) | Immediate relief | Risk of motor weakness and numbness [12] |
These methods are most effective for classic trigeminal neuralgia, which presents as short, electric-shock-like bursts of pain. They are less effective for atypical cases, such as constant burning pain, which may even worsen after treatment [11]. A rare but serious complication called anaesthesia dolorosa – persistent pain in a numb area – can occur, though it is uncommon [12][6]. Major complications like stroke are exceedingly rare, affecting fewer than 1% of cases [12].
Patients are encouraged to discuss their surgeon’s experience, including the number of procedures performed annually and success rates, as these factors can significantly influence outcomes [11].
sbb-itb-2be92ed
Surgical Treatments for Severe Cases
When less invasive methods fall short, surgery becomes a potential option for managing severe trigeminal neuralgia (TN). These procedures are generally reserved for individuals who experience persistent, debilitating pain and are healthy enough to undergo more intensive treatments.
Microvascular Decompression
Microvascular Decompression (MVD) is widely regarded as the top surgical option for classic TN [5]. This procedure involves creating a small opening in the skull under general anaesthesia. The surgeon identifies the blood vessel – most often the superior cerebellar artery – that is pressing against the trigeminal nerve and inserts a soft cushion, typically made of shredded Teflon, to alleviate the pressure [11].
The results are promising: between 80% and 91% of patients experience immediate pain relief [12]. Long-term outcomes are also encouraging, with 70% to 80% remaining pain-free a decade later. However, pain can return for about 10% of patients within the first two years, and the recurrence rate is estimated at 1% to 2% per year [11][12]. Neurosurgeon Kim J. Burchiel emphasises the unique benefits of this approach:
"The MVD is the only surgery where there’s evidence that long‐lasting relief is possible" [11].
As with any brain surgery, MVD carries risks. The combined chance of stroke or death is approximately 2% [12], and other complications may include hearing loss, cerebrospinal fluid leaks, or infection [5].
The surgeon’s experience plays a crucial role in the procedure’s success. Experts recommend choosing a specialist who performs 30 to 50 MVD surgeries annually [11]. Burchiel warns:
"A person who does only two [MVDs] a year doesn’t have enough experience. Just rubbing the nerve could give you six years pain free even though the surgeon missed the real problem" [11].
Interestingly, age is not a strict barrier for MVD. Most neurosurgeons (93.7%) agree that overall health is a better indicator of whether someone is a good candidate for the surgery [13].
Gamma Knife Radiosurgery

Gamma Knife radiosurgery (also called stereotactic radiosurgery or SRS) offers a non-invasive alternative for patients who cannot undergo open surgery or stop taking blood thinners safely [12]. This outpatient procedure uses precisely targeted radiation beams to create a lesion on the trigeminal nerve, disrupting pain signals without the need for incisions or general anaesthesia [11].
While less invasive, Gamma Knife radiosurgery is not as effective as MVD and provides delayed pain relief. Initially, 66% to 85% of patients report pain reduction [5]. However, relief often takes time – typically 2 to 4 weeks, and sometimes up to 2 to 6 months [11][12]. Over time, the success rate diminishes, with about 60% remaining pain-free at 3 years and only 30% to 45% at 10 years [5].
The most common side effect is facial numbness, which affects 18% to 28% of patients, while 4.1% experience severe or bothersome numbness [15]. Neurosurgeon Benjamin Jonker highlights the trade-offs:
"MVD remains the most effective procedure for trigeminal neuralgia… SRS (radiosurgery) is less effective, but the majority still obtain pain relief and it has a very low complication rate" [14].
| Feature | Microvascular Decompression (MVD) | Gamma Knife Radiosurgery (SRS) |
|---|---|---|
| Invasiveness | Invasive (craniotomy) | Non-invasive (radiation) |
| Anaesthesia | General anaesthesia required | None required |
| Initial Success | 80–91% | 66–85% |
| Onset of Relief | Immediate | Delayed (weeks to months) |
| 10-Year Success | 70–80% | 30–45% |
| Common Risks | Hearing loss, cerebrospinal fluid leak, infection | Facial numbness, sensory changes |
Lifestyle and Complementary Approaches
Managing trigeminal neuralgia often involves adapting daily habits in addition to following prescribed clinical treatments. These changes can help reduce the frequency and intensity of pain episodes, offering a more rounded approach to managing this condition.
Avoiding Triggers and Dietary Adjustments
Everyday activities like talking, smiling, or even brushing your teeth can sometimes trigger intense pain episodes for those with trigeminal neuralgia [1]. Even something as simple as a light breeze can provoke discomfort. Adjusting your diet can also play a role in reducing strain on the trigeminal nerve. For instance, sticking to soft foods and avoiding extreme temperatures – whether hot or cold – can help minimise irritation [1]. Foods that require heavy chewing should be avoided to reduce the risk of triggering pain.
Some patients may even experience significant weight loss because they avoid eating altogether to prevent attacks [3]. Protecting your face from cold weather or wind by wearing appropriate clothing can also help [16]. Similarly, small changes to your hygiene routine, like using a soft-bristled toothbrush or rinsing with lukewarm water, can reduce discomfort during everyday tasks. These simple adjustments can make a noticeable difference.
Stress Reduction and Physical Therapy
Stress is another factor that can exacerbate trigeminal neuralgia symptoms. The fear of future pain episodes, combined with the chronic nature of the condition, can lead to anxiety or depression [1]. Mindfulness practices, yoga, and biofeedback are useful tools for managing stress. Gentle activities, such as walking, can boost overall wellbeing without triggering pain [1].
Chronic pain specialist Arun Aggarwal from RPAH Pain Management Centre highlights the value of psychological support:
"Nonpharmacological therapies, such as cognitive behavioural therapy and counselling, may help patients with TN to develop strategies to better manage their pain" [7].
Cognitive Behavioural Therapy (CBT) or counselling can provide patients with coping mechanisms, offering emotional relief alongside physical pain management [1]. These therapies not only address the mental toll of the condition but also empower patients to regain a sense of control over their lives.
Conclusion
Trigeminal neuralgia can be a tough condition to live with, but there are various ways to manage it effectively. Medications like carbamazepine are often the go-to choice for initial treatment, while minimally invasive options – such as glycerol injections or balloon compression – can offer temporary relief when medications don’t work. For those with severe or persistent symptoms, surgical procedures like microvascular decompression can deliver longer-term relief with a low chance of recurrence. On top of medical treatments, making lifestyle changes – like avoiding triggers, managing stress, and seeking psychological support – can go a long way in improving day-to-day life.
Since every patient’s experience with trigeminal neuralgia is different, treatment plans need to be tailored to suit individual needs. There’s no one-size-fits-all solution. Regular reviews are essential to ensure that the chosen approach remains effective, whether that means adjusting medications or considering surgical options as the condition progresses.
If facial pain worsens or basic painkillers aren’t helping, seeing a GP early is critical. From there, your doctor can refer you to specialists – like neurologists, neurosurgeons, or pain management experts – who can work with you to create a treatment plan that fits your specific situation.
FAQs
What are the common side effects of carbamazepine when used to treat trigeminal neuralgia?
Carbamazepine is a medication often used to help manage trigeminal neuralgia, but like many medications, it can come with side effects. Some of the more common ones include drowsiness, dizziness, nausea, and a sense of unsteadiness. Occasionally, people might develop a rash, experience changes in liver function, or have low sodium levels (hyponatraemia).
While rare, there are more serious potential side effects, such as bone marrow suppression, which require immediate attention.
If you experience anything out of the ordinary while taking carbamazepine, it’s crucial to reach out to your healthcare professional. They can help ensure your treatment stays both safe and effective.
What are the differences between minimally invasive treatments and surgery for managing trigeminal neuralgia?
Minimally invasive treatments for trigeminal neuralgia aim to ease pain while causing minimal disruption to surrounding tissues. Techniques like radiosurgery are often preferred because they don’t require incisions, involve shorter recovery times, and come with fewer risks. That said, these methods might need to be repeated if the pain resurfaces.
On the other hand, surgical options such as microvascular decompression (MVD) take a more direct approach. This involves a more invasive procedure performed under general anaesthesia to relieve pressure on the nerve, often caused by nearby blood vessels. While surgery can offer long-term relief, it carries greater risks and demands a longer recovery period. Choosing the right treatment depends on your specific condition, overall health, and personal preferences. Consulting a specialist is the best way to determine the most suitable path forward.
What lifestyle changes can help ease trigeminal neuralgia symptoms?
Lifestyle changes can play a key role in managing trigeminal neuralgia, helping to lessen both the frequency and severity of pain episodes. Simple steps like avoiding triggers – such as abrupt facial movements, cold air exposure, or overexertion of facial muscles – can make a noticeable difference. Stress is another factor that can amplify nerve pain, so incorporating relaxation techniques, mindfulness, or gentle exercise into your routine may help keep it in check.
Other adjustments, like eating a balanced diet, ensuring proper rest, and cutting back on caffeine or alcohol, can support overall nerve health. Paying attention to oral hygiene and steering clear of activities that irritate your face are also important. Working closely with your healthcare provider to combine these lifestyle shifts with medical treatments can lead to better symptom management and an improved quality of life.
Related Blog Posts
- Neurostimulation: Future of Dental Pain Relief
- Antidepressants in Orofacial Pain: Evidence Summary
- Neuropathic Orofacial Pain: Adjuvant Analgesic Options
- Emerging Therapies in Orofacial Pain Management
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





