







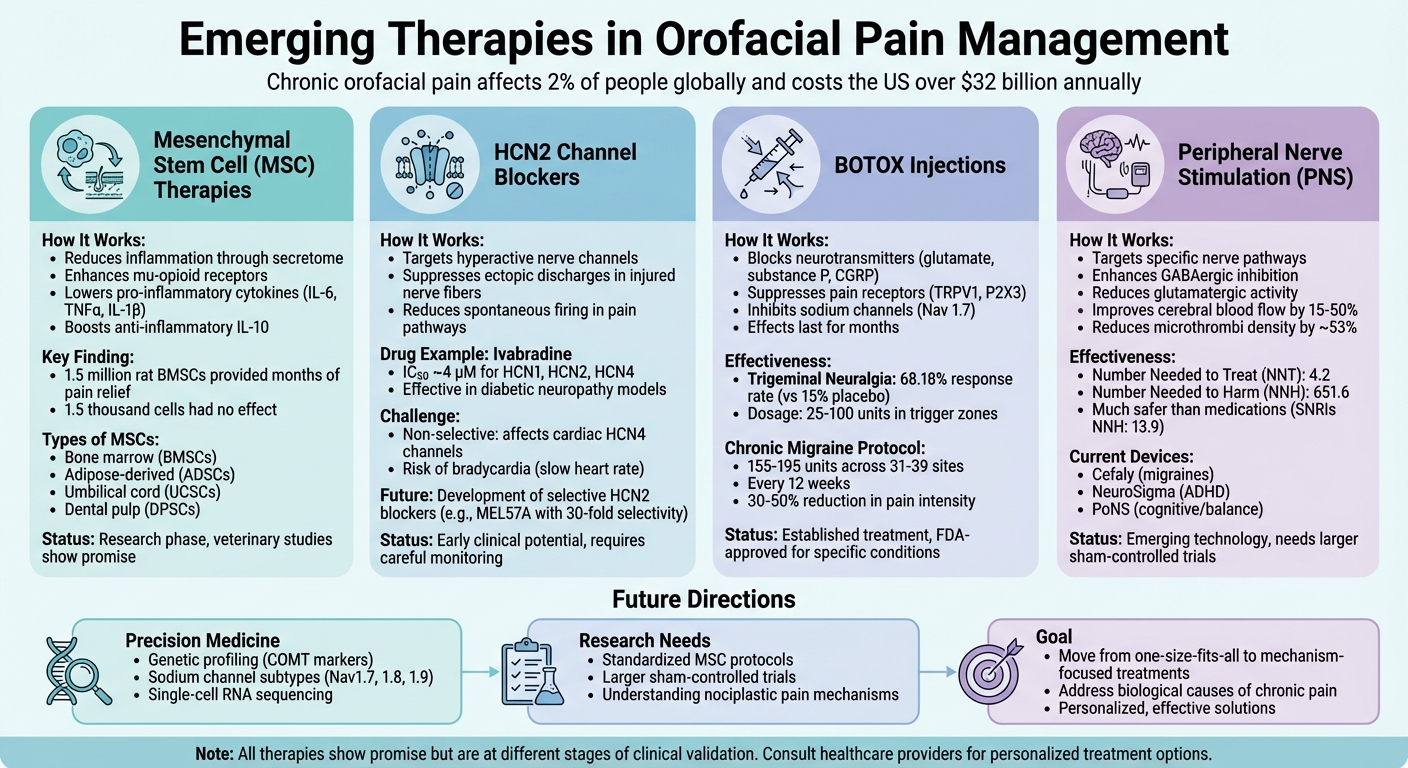
Emerging Therapies in Orofacial Pain Management
Chronic orofacial pain (COFP) affects up to 2% of people globally, disrupting daily activities like speaking, chewing, and emotional expression. Current treatments often fail to address the root causes, leaving many patients with ongoing pain and emotional distress. This article explores new therapies that target the biological mechanisms of COFP, offering potential solutions for long-term relief.
Key Highlights:
- Mesenchymal Stem Cells (MSCs): These cells reduce inflammation and modulate pain through their secretome, showing promise in conditions like temporomandibular joint (TMJ) disorders.
- HCN2 Channel Blockers: These drugs target hyperactive nerve channels, with ivabradine showing early potential despite risks like bradycardia.
- BOTOX Injections: Effective for trigeminal neuralgia and migraines by blocking pain signals at the source.
- Peripheral Nerve Stimulation (PNS): A targeted approach to adjust pain pathways, though more robust research is needed.
Emerging Trends:
- New therapies focus on personalised approaches, targeting specific pain mechanisms.
- Advances in genetic profiling and molecular research could refine treatment options.
- Large-scale trials are critical to validate these therapies for broader use.
These developments aim to provide more effective and tailored solutions for managing COFP, a condition costing the US over $32 billion annually.
Comparison of Emerging Therapies for Chronic Orofacial Pain Management
Mesenchymal Stem Cell Therapies
Mesenchymal stem cell (MSC) therapies are gaining attention as a potential way to manage chronic orofacial pain through neuroimmune modulation.
Types of MSCs Used in Pain Management
MSCs can be sourced from various tissues, each offering unique benefits and limitations. Bone marrow stem cells (BMSCs) are widely studied for their role in bone and cartilage repair, particularly in temporomandibular joint (TMJ) treatments. However, their collection process is invasive, and their slower growth rate can be a drawback [2].
Adipose-derived stem cells (ADSCs) present a more accessible option. These cells, obtained through liposuction, yield higher numbers and grow faster than BMSCs. However, the effectiveness of ADSCs in pain relief can depend on the isolation process used [2]. Umbilical cord stem cells (UCSCs), collected from discarded umbilical tissue, show rapid growth, but their viability varies, with yields ranging between 29% and 63% [2]. Meanwhile, dental pulp stem cells (DPSCs) stand out due to their neural crest origin, which provides enhanced neuroprotective and regenerative capabilities. Extracted from teeth, DPSCs produce high levels of neurotrophic factors, which are crucial for nerve health [2].
These differences highlight the versatility of MSCs and their potential in pain management.
How MSCs Work to Reduce Orofacial Pain
MSCs alleviate pain through anti-inflammatory and immunomodulatory actions. They help regulate chemical signals in the nervous system by lowering levels of pro-inflammatory cytokines like IL-6, TNFα, and IL-1β, while boosting the anti-inflammatory cytokine IL-10 in areas like the trigeminal ganglion and spinal cord [2].
Additionally, MSCs activate the body’s natural pain control mechanisms. They enhance the expression of mu-opioid receptors (MOR) in the rostral ventromedial medulla (RVM), a key area involved in pain inhibition [2].
A significant part of their therapeutic effect comes from the MSC secretome – a mix of proteins, growth factors, and extracellular vesicles they release. This paracrine activity suggests that even cell-free MSC preparations could provide pain relief, while potentially minimising risks such as tumour formation or unintended cell migration [2] [3].
Research Evidence for MSC Therapies
Research supports the idea that MSC dosage plays a critical role in pain relief. A 2011 study at the University of Maryland demonstrated that a single intravenous dose of 1.5 million rat BMSCs significantly reduced mechanical hypersensitivity in rats with masseter muscle tendon ligation. The pain relief lasted several months, whereas a much smaller dose of 1.5 thousand cells had no effect. Interestingly, the study also found that BMSCs cultured beyond 20 passages lost their pain-relieving properties [2].
Veterinary studies further back these findings. For example, adipose-derived MSCs have been shown to reduce pain in dogs suffering from hip osteoarthritis. Researchers are also investigating ways to enhance MSC efficacy, such as "priming" the cells with pro-inflammatory cytokines or exposing them to low-oxygen environments before use [2].
HCN2 Channel Blockade for Pain Relief
Hyperpolarisation-activated cyclic nucleotide-gated (HCN) channels are emerging as a key focus in treating chronic orofacial pain, especially in cases where conventional methods fall short. The growing evidence highlights the importance of precisely targeting HCN channels to achieve better pain relief.
The Role of HCN2 Channels in Orofacial Pain
HCN channels play a pivotal role in regulating neuronal excitability within the trigeminal pathway – the primary nerve network responsible for facial sensation and pain [5]. When the trigeminal nerve is injured, the Ih current density in ganglion neurons increases. This triggers ectopic discharges in injured Aδ and Aβ fibres, leading to cross-excitation. Essentially, this means that injured fibres can activate nearby healthy ones, resulting in conditions like allodynia and hyperalgesia [5]. This phenomenon can sometimes cause neuropathic pain to be mistaken for dental pain, delaying proper diagnosis and treatment [5].
"Resolving this mechanistic ambiguity is critical for preventing pain chronification and developing more effective, personalised therapeutic strategies." [1]
Studies have shown that blocking Ih currents can completely suppress ectopic discharges in Aβ fibres in rat models of nerve injury-induced neuropathic pain. Additionally, it reduces spontaneous firing in Aδ fibres [5]. While HCN channels in healthy neurons regulate rhythmic activity, their overexpression in chronic pain conditions leads to hyperexcitability, sustaining persistent pain signals [5][6]. These findings suggest that selective HCN2 blockers could offer targeted relief.
Ivabradine as a Treatment Option
Ivabradine, a non-selective HCN blocker, has shown promise in reducing mechanical hypersensitivity in animal models. This drug (IC50 ~4 µM for HCN1, HCN2, and HCN4) has demonstrated effectiveness in managing mechanical hypersensitivity in diabetic neuropathy models [8]. Research led by David Ramírez highlighted ivabradine’s ability to reduce chronic pain in mice, with the team suggesting that "selective HCN2 inhibitors might be a valuable treatment strategy for diabetic neuropathies" [8].
However, the lack of isoform selectivity in current HCN blockers like ivabradine poses challenges. By also affecting cardiac HCN4 channels, these drugs carry the risk of bradycardia [7][8]. This is particularly concerning because HCN4 is predominantly expressed in human heart tissue [7]. As a result, clinicians prescribing ivabradine off-label for pain management must carefully monitor heart rate [7].
The focus is now shifting toward developing medications that are more precise. Researchers are working on isoform-selective blockers that specifically target HCN2 channels in the nervous system while avoiding HCN4 channels in the heart [8][1]. Experimental compounds like MEL57A have shown up to 30-fold selectivity for HCN1 over HCN2, paving the way for more targeted therapies in the future [7][8].
| HCN Isoform | Primary Location | Role in Body | Sensitivity to cAMP |
|---|---|---|---|
| HCN1 | Brain, Peripheral Nerves | Neuronal excitability, pain | Weak [8] |
| HCN2 | CNS, Nociceptors | Neuropathic/Inflammatory pain | High [8] |
| HCN3 | Brain (low levels), CNS | Neuronal excitability | Absent [8] |
| HCN4 | Heart (Sinoatrial node) | Cardiac pacing (heart rate) | High [7][8] |
BOTOX and Neuromodulator Injections
BOTOX isn’t just for cosmetic treatments – it offers a powerful option for managing chronic orofacial pain, especially when other treatments fall short. Botulinum toxin type A (BoNT-A) works by interrupting pain signals on both peripheral and central levels. For patients who struggle with systemic side effects from medications like carbamazepine (dizziness occurs in roughly 40% of users), BOTOX provides a more targeted, localised alternative [10][11].
How BOTOX Reduces Pain
BOTOX tackles pain by disrupting the release of neurotransmitters like glutamate, substance P, and CGRP from sensory neurons. This disruption is achieved by interfering with SNARE-mediated neurotransmitter release. Essentially, it blocks pain signals at their source and even modulates central pathways through retrograde transport [10][11][12].
"BoNT-A exerts analgesic effects across the spectrum of orofacial pain disorders via dual mechanisms, segmental neural blockade and retrograde axonal transport leading to central neuromodulation." – Yair Sharav, Department of Oral Medicine, Hadassah Medical Centre [10]
Beyond this, BOTOX also suppresses pain-related sensory receptors like TRPV1 and P2X3, while inhibiting sodium channels (e.g., Nav 1.7) that are crucial for pain signalling [10][12]. The effects of a single treatment can last for months, making it an appealing alternative to daily medication regimens [10].
Treatment Protocols and Expected Outcomes
BOTOX’s ability to target specific pain pathways makes it a predictable and effective option for many. For trigeminal neuralgia, injections are delivered subcutaneously, intradermally, or submucosally into identified trigger zones. Dosages typically range from 25 to 100 units, diluted to 5 U per 0.1 mL [13].
In a study conducted at the Hadassah Medical Centre in August 2025, 42 patients with trigeminal neuralgia were treated with 75 U of BoNT-A diluted in 2 mL of saline. After 12 weeks, 68.18% of the BOTOX group showed a positive response, compared to just 15.00% in the placebo group [13].
For chronic migraines, the PREEMPT protocol is used. This involves injecting 155 to 195 units across 31 to 39 specific sites every 12 weeks [10][14]. Success is measured by tracking headache frequency and pain intensity using the Visual Analogue Scale (VAS). Patients are considered responders if they achieve a 30% to 50% reduction in pain intensity [13][14]. While side effects like facial asymmetry or localised weakness can occur, they are usually mild and temporary [10][11].
| Condition | Injection Site | Typical Dosage | Primary Outcome |
|---|---|---|---|
| Trigeminal Neuralgia | Trigger zones (intradermal/mucosal) | 25 U – 100 U | 65–90% response rate; reduced attack frequency |
| Chronic Migraine | 31–39 sites (PREEMPT protocol) | 155 U – 195 U | Reduction in headache days per month |
| Myofascial Pain | Masseter and temporalis muscles | 25 U – 50 U per site | Reduced muscle tenderness and referred pain |
Patients often need 2–3 treatment cycles before determining if the therapy is effective. Improvements may take time to become apparent, but this method is particularly helpful for older patients who can’t tolerate the side effects of systemic medications or aren’t suitable for invasive surgeries [11].
sbb-itb-2be92ed
Peripheral Nerve Stimulation for Neuropathic Pain
When medications and injections fall short, peripheral nerve stimulation (PNS) offers a targeted alternative for managing chronic orofacial neuropathic pain. Unlike systemic drugs that affect the entire body, PNS hones in on specific nerve pathways to directly adjust pain signals. This precise approach opens up new possibilities for understanding its mechanisms.
How Peripheral Nerve Stimulation Works
PNS, particularly trigeminal nerve stimulation (TNS), focuses on sensory nerve fibres and activates critical brainstem nuclei like the medullary dorsal horn and trigeminal spinal subnucleus caudalis [16][17]. It achieves pain relief by enhancing GABAergic inhibition, reducing glutamatergic and NMDA receptor activity, and promoting the release of neuropeptides such as CGRP, Substance P, and nitric oxide. These neuropeptides not only encourage vasodilation but also help reduce inflammation [17].
"TNS harnesses the release of vasoactive neuropeptides, modulation of neurotransmission, and direct action upon the autonomic nervous system to generate a suite of powerful multitarget therapeutic effects." – Bioelectronic Medicine [17]
Additionally, PNS plays a role in lowering microglial activation and suppressing cytokines like TNF‑α and IL‑1β [17]. It also improves cerebral blood flow by 15–50%, reduces microthrombi density by around 53%, and helps regulate neural plasticity to combat "memorised pain" [1].
Current Research and Potential Applications
PNS represents an exciting development in neuroimmune modulation for managing orofacial pain. While research into its applications is growing, larger sham-controlled trials are needed to confirm its long-term effectiveness and safety [9]. In late 2024, the American Society of Interventional Pain Physicians published detailed guidelines for implantable PNS in chronic pain management, focusing on patient selection and procedural safety [18]. Current uses include occipital nerve stimulation for chronic migraines and sphenopalatine ganglion neurostimulation for trigeminal neuralgia [15].
A 2025 meta-analysis of 313 trials involving over 48,000 participants revealed that neuromodulation techniques, such as repetitive transcranial magnetic stimulation, have a number needed to treat (NNT) of 4.2 – similar to first-line medications like tricyclic antidepressants (NNT 4.6) [9]. Importantly, the number needed to harm (NNH) for neuromodulation is significantly higher at 651.6, indicating a much lower likelihood of treatment discontinuation due to side effects compared to drugs like SNRIs (NNH 13.9) or tricyclic antidepressants (NNH 17.1) [9].
"TNS research indicates that it is at a tipping point, with the capacity to emerge as a leading treatment, potentially poised to become as widespread as vagus nerve stimulation (VNS)." – Bioelectronic Medicine [17]
Several TNS-based devices are already available, including Cefaly for migraines, NeuroSigma for paediatric ADHD, and PoNS for cognitive and balance disorders [17]. However, the evidence supporting PNS for chronic orofacial pain (excluding headaches) remains limited. Many studies fail to fully account for placebo effects [15]. These early findings highlight the need for more robust research, particularly large sham-controlled trials, to establish PNS as a dependable option for managing orofacial pain. For now, treatment outcomes remain modest, underscoring the importance of further investigation [9].
Conclusion and Future Directions
Key Points from New Therapies
Orofacial pain management is evolving from one-size-fits-all methods to more precise, mechanism-focused treatments aimed at addressing the biological causes of chronic pain [1][4]. For instance, mesenchymal stem cells (MSCs) and their secretome show potential for long-term immunomodulation by enhancing mu-opioid receptors and rebalancing cytokines [2]. Research into HCN2 channels highlights their role in reducing abnormal discharges in injured nerve fibres [5]. Meanwhile, BOTOX injections have demonstrated their ability to block pro-nociceptive neurotransmitter release, particularly in cases like trigeminal neuralgia [5][15]. Peripheral nerve stimulation is another promising technique, with early evidence suggesting it can modulate pain signals, though additional studies are needed to refine its use [1][5]. Collectively, these developments pave the way for more personalised and effective treatment options.
What’s Next in Orofacial Pain Management
The next wave of advancements aims to bridge the gap between clinical symptoms and their biological underpinnings [1]. Precision medicine, driven by genetic profiling, could play a key role. Markers like COMT and sodium channel subtypes (Nav1.7, 1.8, and 1.9) may help identify patients who would benefit most from specific neuroimmune or ion-channel-targeted therapies [4]. Emerging technologies such as single-cell RNA sequencing and spatial transcriptomics could provide detailed maps of molecular changes in the trigeminal ganglion, particularly during the shift from acute to chronic pain [1].
MSCs continue to show promise, with their conditioned media and exosomes offering possibilities for standardised dosing and enhanced safety [2]. However, to fully realise these therapies, researchers need to address several gaps. For example, standardised protocols for secretome collection, larger sham-controlled trials for neuromodulation techniques, and a deeper understanding of nociplastic pain mechanisms are essential [2][15][1].
With chronic orofacial pain affecting around 20% of the US population and costing over US$32 billion annually, these emerging therapies offer a pathway to more effective, tailored treatments [2]. The challenge now lies in refining these approaches through rigorous research and clinical trials.
FAQs
How can mesenchymal stem cells help manage chronic orofacial pain?
Mesenchymal stem cells (MSCs) offer a promising way to address chronic orofacial pain by aiding nerve repair and easing inflammation. These cells stand out for their ability to regenerate damaged tissues and regulate neuroinflammatory responses – both key factors in managing persistent pain.
In cases like trigeminal neuralgia or temporomandibular joint disorders, MSCs contribute to nerve healing by restoring proper neural function. They also help alleviate chronic pain by regulating cytokine activity and minimising the activation of glial cells, which are often involved in extended inflammation. This non-opioid treatment approach presents a valuable option for tackling complex orofacial pain conditions.
What are the possible side effects of using HCN2 channel blockers like ivabradine for orofacial pain management?
HCN2 channel blockers like ivabradine can sometimes lead to side effects such as visual disturbances, bradycardia (a slower-than-normal heart rate), and possible heart rhythm issues. These reactions happen because the medication affects both the heart and the visual system.
Before beginning any treatment, it’s crucial to speak with a healthcare professional. They can help determine if the medication is appropriate for your condition and explain any potential risks involved.
Can BOTOX help manage trigeminal neuralgia and migraines effectively?
BOTOX (botulinum toxin type A) has shown promise in managing conditions like trigeminal neuralgia and migraines. Its pain-relieving effects are tied to its ability to reduce inflammation and influence nerve signalling, which can ease chronic pain.
Recent developments in treatment suggest that BOTOX can be effective either as a standalone therapy or when combined with other treatments. It offers a minimally invasive option with potential for long-term relief. However, results can differ from person to person, making it crucial to consult a healthcare professional to determine if it’s a suitable choice for your specific needs.
Related Blog Posts
- Neurostimulation: Future of Dental Pain Relief
- Studies on Pain Management in Dental Extractions
- Emerging Biomarkers in Orofacial Pain Research
- Antidepressants in Orofacial Pain: Evidence Summary
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





