







Neuropathic Orofacial Pain: Adjuvant Analgesic Options

Neuropathic orofacial pain, like trigeminal neuralgia or burning mouth syndrome, stems from nerve dysfunction rather than dental issues. It often feels like burning, electric shocks, or tingling and can disrupt daily life. Standard painkillers (e.g., paracetamol) usually don’t work, so treatments focus on adjuvant analgesics – medications originally designed for other conditions but effective for nerve pain.
Key treatment options include:
- Anticonvulsants (e.g., gabapentin, carbamazepine): Calm overactive nerves.
- Antidepressants (e.g., amitriptyline, duloxetine): Alter pain pathways.
- Topical treatments (e.g., lidocaine): Target localised pain.
Doctors and dentists collaborate to diagnose and manage these conditions, ensuring treatments are tailored to individual needs. Regular monitoring is crucial for adjusting medications and minimising side effects.
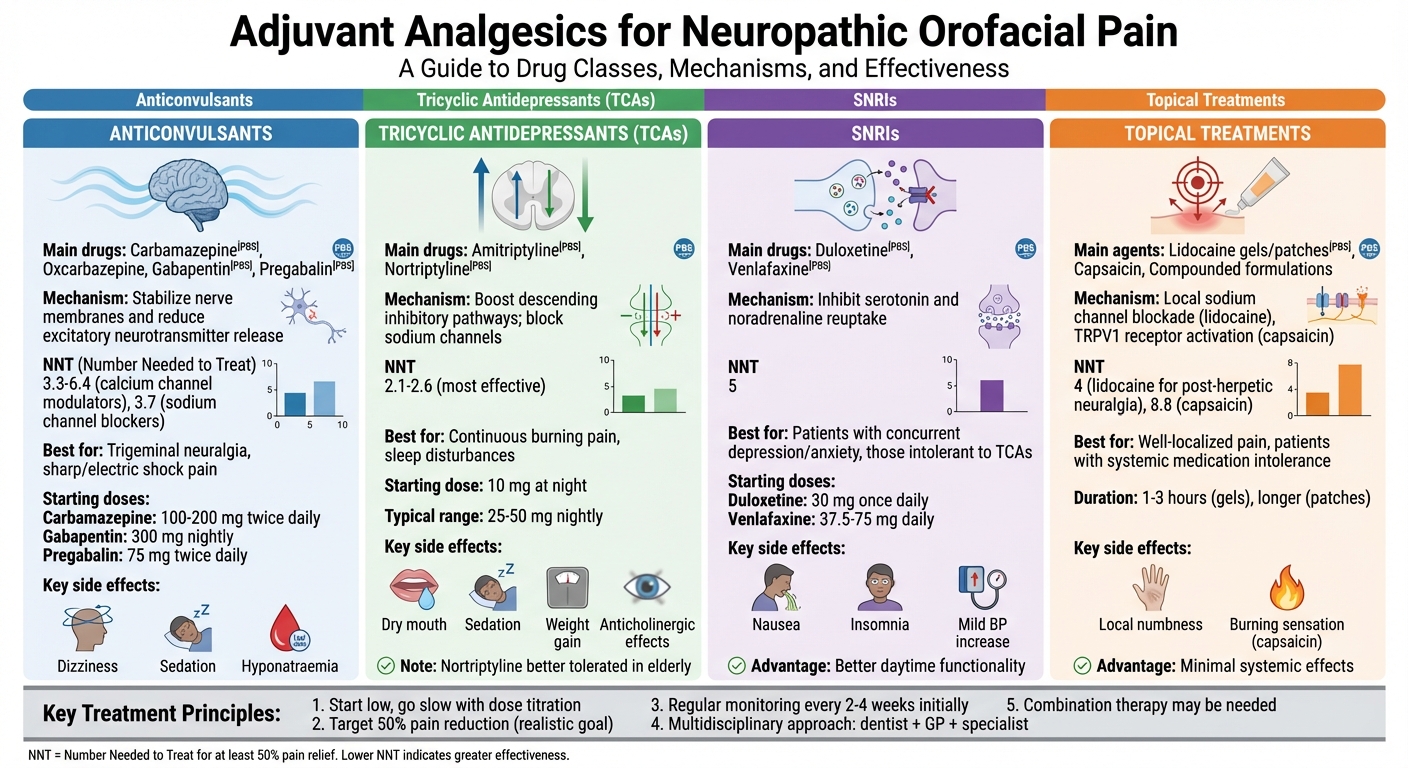
Adjuvant Analgesics for Neuropathic Orofacial Pain: Drug Classes Comparison
How Adjuvant Analgesics Work
Treatment Goals
Adjuvant analgesics aim to ease pain and improve daily activities like speaking, chewing, and maintaining oral hygiene [4]. While complete pain relief is uncommon, achieving a 50% reduction can significantly enhance orofacial function, improve sleep and mood, and reduce the need for opioids [4]. Let’s take a closer look at how these medications work to manage pain.
How These Medications Target Pain
Neuropathic pain stems from overactive nerves sending pain signals, even when there’s no tissue damage [4]. Different classes of adjuvant analgesics tackle this abnormal nerve activity in unique ways:
- Sodium channel blockers (e.g., carbamazepine, oxcarbazepine): These stabilise nerve membranes by blocking voltage-gated sodium channels, reducing irregular nerve firing, particularly in conditions like trigeminal neuralgia [4].
- Calcium channel modulators (e.g., gabapentin, pregabalin): These bind to nerve cells to limit the release of excitatory neurotransmitters like glutamate and substance P, which helps reduce central sensitisation [4].
- Tricyclic antidepressants and SNRIs (e.g., duloxetine): These enhance pain inhibition by increasing serotonin and noradrenaline levels. Tricyclics may also block sodium channels, while SNRIs generally cause fewer anticholinergic side effects [4].
These mechanisms contribute to better pain control, improved function, and enhanced quality of life for patients [4].
| Drug Class | Main Mechanism | Typical NNT* |
|---|---|---|
| Tricyclic antidepressants (e.g., amitriptyline) | Boost descending inhibitory pathways; block sodium channels | 2.1–2.6 [4] |
| Sodium channel blockers (e.g., carbamazepine) | Suppress ectopic nerve firing in trigeminal pathways | 3.7 [4] |
| Calcium channel modulators (e.g., pregabalin, gabapentin) | Reduce excitatory neurotransmitter release | 3.3–6.4 [4] |
| SNRIs (e.g., duloxetine) | Inhibit serotonin and noradrenaline reuptake | 5 [4] |
*NNT = Number Needed to Treat for at least 50% pain relief
Prescribing in Australia
In Australia, prescribing adjuvant analgesics follows strict Therapeutic Goods Administration (TGA) protocols. Medications like gabapentin, pregabalin, carbamazepine, and amitriptyline are included in the Pharmaceutical Benefits Scheme (PBS) for neuropathic pain, though some require specialist approval [3].
Doctors typically start with low doses (e.g., gabapentin 300 mg daily, increasing to a maximum of 3,600 mg per day) and gradually adjust over days or weeks to balance pain relief with side effects like dizziness, sedation, or nausea [3]. Regular follow-ups are critical to assess pain levels, functional improvements (like chewing or speaking), and any adverse effects [7].
For carbamazepine, additional monitoring is necessary, including periodic blood tests to maintain therapeutic levels (4–12 mg/L) and checks on kidney, liver, and blood function [7]. Reviews are usually scheduled every 2 to 4 weeks during the initial phase and every 3 to 6 months once the treatment stabilises, in line with Therapeutic Guidelines and PBS rules [7].
Facial Pain: A Treatment Matrix – Won Kim, MD | UCLA Neurosurgery

Anticonvulsants for Neuropathic Orofacial Pain
Anticonvulsants help calm overactive nerve pathways responsible for transmitting pain signals. The choice of medication often depends on whether the pain is episodic and sharp or continuous and burning. Below, we explore key options for managing both types of neuropathic pain.
Carbamazepine and Oxcarbazepine
Carbamazepine is a go-to treatment for classical trigeminal neuralgia, showing an initial success rate of about 70–80% [2][3]. It works by blocking voltage-gated sodium channels in the trigeminal nerve, dampening the abnormal nerve activity that causes sudden facial pain. In Australia, treatment generally starts at 100–200 mg twice daily, with doses gradually adjusted based on the patient’s response and tolerance.
Oxcarbazepine, which works similarly, is often preferred for its lower risk of drug interactions and better tolerability in older adults. However, it comes with a risk of hyponatraemia, making regular electrolyte monitoring essential.
Both drugs require careful monitoring. Baseline and periodic checks typically include full blood counts, liver function tests, and electrolyte levels. Additionally, patients from certain ethnic groups may need genetic testing (e.g., HLA-B*1502 screening) before starting carbamazepine to minimise the risk of severe skin reactions.
| Aspect | Carbamazepine | Oxcarbazepine |
|---|---|---|
| Initial Dose | 100–200 mg twice daily | 300 mg twice daily |
| Effectiveness | 70–80% response in trigeminal neuralgia | Similar efficacy; fewer interactions |
| Main Side Effects | Dizziness, rash, blood issues | Hyponatraemia, dizziness |
| Monitoring Required | Blood counts, liver tests, genetic screening | Sodium levels, liver tests |
| PBS Subsidy | Yes, for neuropathic pain | Yes, for neuropathic pain |
Gabapentin and Pregabalin
If carbamazepine doesn’t work or isn’t suitable, gabapentin and pregabalin are excellent alternatives. These drugs target the α2δ subunit of voltage-gated calcium channels, reducing the release of excitatory neurotransmitters. They’re particularly helpful for continuous neuropathic pain, such as post-traumatic trigeminal neuropathy.
Gabapentin typically starts at 300 mg at night, with doses gradually increased to between 900 and 3,600 mg daily, split into multiple doses. Around 40% of users experience significant pain reduction. Pregabalin, which acts faster and requires fewer daily doses, begins at 75 mg twice daily and can be increased to a maximum of 600 mg daily. However, pregabalin has a higher potential for misuse. Both medications are approved by the Therapeutic Goods Administration (TGA) and subsidised under the PBS, though pregabalin often requires authority approval.
| Aspect | Gabapentin | Pregabalin |
|---|---|---|
| Starting Dose | 300 mg nightly | 75 mg twice daily |
| Maximum Daily Dose | Up to 3,600 mg | Up to 600 mg |
| Effectiveness | 30–50% pain reduction | Approximately 50% response in trials |
| Dosing Frequency | Three times daily | Twice daily |
| Common Side Effects | Drowsiness, dizziness, weight gain | Similar side effects; higher misuse potential |
| Bioavailability | Dose-dependent | More predictable |
Additional Anticonvulsant Options
For patients who don’t find relief with first-line anticonvulsants, options like lamotrigine, topiramate, and baclofen can be considered as add-ons. Lamotrigine inhibits sodium channels and reduces glutamate release, making it a useful complement in cases resistant to carbamazepine. Topiramate, which affects multiple ion channels, may also help and has the added benefit of potential weight loss. Baclofen, a GABA-B agonist, works by lowering overall nerve excitability.
The evidence supporting these additional drugs is limited, relying mostly on small case studies and expert opinions rather than robust clinical trials. In Australia, these medications are typically used off-label, and patients should have realistic expectations about their effectiveness. Dentists can play a crucial role in identifying pain triggers and referring patients to specialists for complex treatment plans.
Antidepressants for Neuropathic Orofacial Pain
When anticonvulsants alone aren’t enough to manage neuropathic orofacial pain, antidepressants can step in as effective alternatives. These medications work on pain pathways independently of their mood-enhancing effects, offering relief even to those without mood disorders. Two main categories – tricyclic antidepressants (TCAs) and serotonin–noradrenaline reuptake inhibitors (SNRIs) – are commonly used, each with its own advantages depending on the patient’s needs and tolerance. Below, we explore how these two classes of antidepressants contribute to managing neuropathic orofacial pain.
Tricyclic Antidepressants
TCAs, such as amitriptyline and nortriptyline, are widely recognised for their ability to relieve neuropathic pain. They do this by blocking the reuptake of serotonin and noradrenaline in descending pain pathways, inhibiting voltage-gated sodium channels, and modulating NMDA receptors involved in central sensitisation [2]. Interestingly, these effects occur at lower doses (10–25 mg at night) than those typically used for treating depression.
The effectiveness of TCAs in neuropathic pain is well-documented. For example, amitriptyline has a number-needed-to-treat (NNT) of about 2.1–2.6, meaning that one in every two to three patients experiences significant pain relief [4]. However, these benefits often come with a higher likelihood of side effects.
Nortriptyline, on the other hand, is generally better tolerated, especially by older adults. It causes less sedation and fewer anticholinergic effects – such as dry mouth, constipation, blurred vision, and urinary retention – making it a safer option for elderly patients or those with cardiovascular concerns [4][6]. Despite these differences, amitriptyline can still be a preferred choice when its sedative effects help manage sleep disturbances often associated with neuropathic facial pain.
Both medications require careful oversight. Initial assessments typically include checking blood pressure, and patients should be monitored for side effects like orthostatic hypotension, weight gain, and cardiac conduction issues, particularly in high-risk individuals. Dry mouth, a common side effect, is of particular concern for dental patients as it can increase the risk of tooth decay and gum disease. Dental clinics, such as Complete Smiles Bella Vista, can play a key role in monitoring these oral health issues and coordinating care with general practitioners. This collaborative approach ensures patients receive comprehensive care that supports both pain relief and oral health.
| Aspect | Amitriptyline | Nortriptyline |
|---|---|---|
| Starting Dose | 10 mg at night | 10 mg at night |
| Typical Analgesic Range | 25–50 mg nightly | 25–50 mg nightly |
| Effectiveness (NNT) | 2.1–2.6 for neuropathic pain | Similar efficacy to amitriptyline |
| Sedation Level | High (helps with sleep issues) | Lower (better for daytime activities) |
| Anticholinergic Effects | More pronounced | Fewer side effects |
| Best Suited For | Patients needing sleep support | Older adults; those with cardiovascular concerns |
Serotonin–Noradrenaline Reuptake Inhibitors
For patients who can’t tolerate TCAs or have concurrent conditions like depression or anxiety, SNRIs – including duloxetine and venlafaxine – offer another option. These medications work by selectively blocking the reuptake of serotonin and noradrenaline [2], providing effective pain relief with a milder side-effect profile.
Although their pain-relieving effects may be slightly less potent than TCAs, with an NNT of approximately 5 for neuropathic pain [4], SNRIs are often better suited for patients who need to maintain daytime functionality. Duloxetine is typically started at 30 mg once daily and increased to 60 mg if well-tolerated, while venlafaxine begins at doses of 37.5–75 mg daily with gradual adjustments [5].
Common side effects of SNRIs include nausea (particularly during the first few weeks), reduced appetite, insomnia or drowsiness, sweating, and mild increases in blood pressure. Venlafaxine, in particular, may require periodic blood pressure monitoring [2]. Because SNRIs cause less dry mouth and sedation compared to TCAs, they are often a better choice for individuals who need to drive, work, or manage cardiovascular concerns.
In Australia, dentists don’t typically prescribe these medications but play a crucial role in identifying neuropathic orofacial pain, explaining treatment options, and referring patients to general practitioners or pain specialists for further management [6][8]. This team-based approach ensures patients receive well-rounded care while maintaining their oral health.
sbb-itb-2be92ed
Topical Treatments for Localised Pain
When pain is restricted to a specific area, topical treatments can be an effective option alongside systemic therapies. For localised neuropathic orofacial pain – like a trigger zone on the gum or inside the cheek – these treatments provide relief directly at the source. This approach is particularly useful for conditions such as post-traumatic trigeminal neuropathy or localised post-herpetic neuralgia. The oral mucosa’s higher permeability allows medications to reach higher concentrations in the affected area, offering targeted relief without the systemic side effects of oral medications[1].
Lidocaine and Compounded Formulations
Lidocaine is a commonly used topical treatment for localised neuropathic facial pain. This local anaesthetic works by blocking voltage-gated sodium channels, stabilising nerve membranes and reducing pain signals[1]. In Australia, lidocaine is available in various forms, including gels, viscous solutions, and transdermal patches that can be trimmed for facial use. For post-herpetic neuralgia, lidocaine patches have shown an NNT (number needed to treat) of approximately 4, meaning one in four patients experiences significant pain relief[4].
Lidocaine gels provide rapid relief within minutes, though the effect typically lasts 1–3 hours. Patches offer longer-lasting relief but may take more time to take effect. Side effects are generally mild, such as temporary numbness and irritation. Patients should be cautious to avoid biting numb areas or consuming hot foods and drinks while using these treatments[1].
For cases where standard lidocaine treatments are insufficient, compounded formulations may be an option. These customised mixtures, prepared by compounding pharmacists, combine lidocaine with other agents such as anticonvulsants, tricyclic antidepressants, clonidine, ketamine, or clonazepam. In one observational study, patients using compounded topical therapies reported an average 40% reduction in pain[1]. While evidence supporting these formulations is limited, they can be beneficial for well-localised pain that doesn’t respond to simpler treatments.
| Aspect | Standard Lidocaine | Compounded Formulations |
|---|---|---|
| Mechanism | Sodium channel blockade | Multiple mechanisms (varies by ingredients) |
| Typical Formulations | Gels, viscous solutions, patches | Custom mixtures with additional agents |
| Onset & Duration | Rapid onset; lasts 1–3 hours (gels) | Varies; often similar to the lidocaine component |
| Evidence Level | Strong evidence for post-herpetic neuralgia (NNT ≈ 4) | Limited evidence from observational studies |
| Common Side Effects | Local numbness, mild irritation | Similar to lidocaine; depends on added agents |
| Availability | Widely available in Australia (PBS-listed) | Requires compounding pharmacy; may add costs |
| Best Suited For | Rapid relief for localised pain | Refractory pain or cases with systemic intolerance |
Dental professionals often collaborate with general practitioners and compounding pharmacists to create tailored topical regimens. Other topical agents, like capsaicin, can also be considered for managing localised pain.
Capsaicin and Other Topical Agents
Capsaicin takes a different approach to pain relief by activating TRPV1 receptors on pain-sensing nerve fibres. This activation initially causes a burning sensation, but over time it desensitises the receptors and decreases pain signals by depleting substance P from nerve endings[1]. Capsaicin is available in low-concentration creams and gels for home use, as well as high-concentration 8% patches applied under medical supervision.
While capsaicin can provide longer-lasting relief, its tolerability is often a concern. The high-concentration patch has an NNT of approximately 8.8, meaning more patients need to be treated for one to experience significant relief compared to lidocaine patches[4]. The initial burning sensation can be intense, but this discomfort usually subsides after a few days to weeks as desensitisation occurs. Capsaicin is best suited for patients with well-defined localised neuropathic pain who can handle the initial discomfort. For those needing immediate relief or who are sensitive to burning sensations, lidocaine remains the preferred choice.
Other topical options include benzocaine, topical NSAIDs like diclofenac (useful when pain has both inflammatory and neuropathic components), and specialised compounds containing agents such as clonidine or ketamine. The choice of treatment depends on factors like pain location, mucosal tolerance, medical conditions, and patient preferences.
Creating Individual Treatment Plans
When it comes to managing neuropathic pain, creating tailored treatment plans is a must. These plans take into account various factors like the specific diagnosis (such as classic trigeminal neuralgia, post-traumatic trigeminal neuropathy, or persistent idiopathic facial pain), the patient’s age, overall health, current medications, and how they’ve responded to treatments in the past.
Choosing the Right Treatment
Selecting the right medication involves balancing several practical considerations. For classic trigeminal neuralgia – characterised by sudden, electric-shock-like pain triggered by touch or chewing – carbamazepine or oxcarbazepine is often the go-to. These medications are known for their ability to calm abnormal nerve activity. On the other hand, for continuous, burning pain that interferes with sleep or mood, options like gabapentin, pregabalin, or low-dose tricyclic antidepressants may be more suitable.
Age and health conditions also play a big role in treatment decisions. Older adults, for instance, are more prone to side effects like dizziness or sedation, so starting with lower doses and gradually increasing them is key. Conditions like cardiovascular disease, glaucoma, or kidney issues might mean avoiding certain drugs altogether or adjusting doses. In cases where systemic risks or multiple medications are a concern, topical treatments like lidocaine gels or compounded formulations can provide targeted relief without the broader risks.
Step-by-Step Treatment Approach
Start with a low dose of the chosen systemic medication, gradually increasing it over four to eight weeks. If the pain persists but improves slightly, consider optimising the dose or introducing a second medication that targets a different pain mechanism. For example, combining gabapentin with a low-dose tricyclic antidepressant can address both nerve hyperactivity and central sensitisation. When these approaches are no longer effective, more advanced options like local anaesthetic nerve blocks or botulinum toxin A injections can be explored with the help of pain or orofacial specialists.
Regular follow-ups are crucial. These appointments help track pain levels, assess daily activities like chewing and sleeping, monitor mood, and check for side effects. If side effects become too much to handle, adjustments can be made – whether that means reducing the dose, switching to another drug in the same class, or trying a medication from a different class. Long-term care may also include gradually simplifying or tapering treatment once the pain is under control, often alongside non-medication strategies like physical therapy, relaxation techniques, or psychosocial support. This structured approach makes it easier to coordinate care with dental professionals.
How Dentists Support Treatment
Dentists play an important role in identifying neuropathic orofacial pain and distinguishing it from dental issues like cavities or gum disease. Neuropathic pain often presents as electric-shock sensations, burning discomfort, or pain triggered by light touch – different from the pain caused by chewing or biting. A thorough clinical and radiographic exam helps rule out dental causes like caries, pulpitis, cracked teeth, or periodontal disease. If no dental issues are found, dentists should consider referring the patient to a general practitioner or an orofacial pain specialist for further evaluation.
Practices like Complete Smiles Bella Vista are skilled at spotting unusual pain patterns, avoiding unnecessary dental procedures, and coordinating specialist referrals. Once a neuropathic pain diagnosis is confirmed, dentists can support the treatment plan by stabilising occlusion, addressing related issues like temporomandibular disorders or bruxism, and steering clear of invasive procedures in affected areas. They also guide patients on avoiding triggers, practising effective self-care, and understanding the gradual nature of medication adjustments. By staying in close communication with the prescribing doctor, dentists ensure their care aligns with the patient’s overall treatment plan.
Summary
Neuropathic orofacial pain doesn’t respond well to standard painkillers like paracetamol or non-steroidal anti-inflammatory drugs. Instead, treatment typically involves adjuvant analgesics such as anticonvulsants, antidepressants, and topical treatments. These medications form the foundation of an effective treatment strategy.
Anticonvulsants like carbamazepine, oxcarbazepine, gabapentin, and pregabalin work by stabilising nerve activity, making them particularly useful for conditions like trigeminal neuralgia. Antidepressants, including TCAs and SNRIs, not only help modulate pain processing in the brain but also provide added benefits for sleep and mood. For targeted relief, topical options such as lidocaine gels or compounded formulations can be applied directly to areas of localised pain.
Achieving the best results requires a coordinated, multidisciplinary approach. This means collaboration between general dentists, general practitioners, orofacial pain specialists, and pain physicians. Such teamwork reduces unnecessary dental procedures and ensures the safe and effective use of adjuvant medications.
Dentists play a crucial role in this model. They are often the first to identify neuropathic pain and distinguish it from common dental issues. By referring patients to GPs or specialists for systemic treatment, dentists set the stage for proper care. Once a diagnosis is made, they continue to support the patient by monitoring oral health and working closely with prescribers before any invasive procedures. Practices like Complete Smiles Bella Vista are well-equipped to provide comprehensive dental care and facilitate specialist referrals, ensuring patients receive the best possible treatment.
FAQs
What side effects can occur with medications used for neuropathic orofacial pain?
Adjuvant analgesics, like anticonvulsants and antidepressants, are often prescribed to help manage neuropathic orofacial pain. While effective, they may occasionally lead to side effects such as dizziness, drowsiness, dry mouth, nausea, or mild stomach discomfort.
If any side effects persist or become severe, it’s crucial to reach out to your healthcare provider. They can evaluate your symptoms and discuss potential alternatives to better suit your needs.
How do healthcare professionals work together to treat neuropathic orofacial pain?
Managing neuropathic orofacial pain often involves teamwork between dentists and medical professionals. Specialists like neurologists or pain management doctors are usually responsible for diagnosing the condition. They might prescribe adjuvant analgesics, such as anticonvulsants or antidepressants, to help control nerve-related pain.
Dentists, on the other hand, focus on identifying and addressing any dental issues that might be contributing to the discomfort. This could include concerns like misaligned teeth or problems with the jaw. They may also provide targeted treatments to alleviate pain. By combining the expertise of both medical and dental professionals, this collaborative approach ensures patients receive comprehensive and personalised care designed to meet their unique needs.
When is it appropriate to use topical treatments for neuropathic orofacial pain?
Topical treatments can be a helpful way to manage neuropathic orofacial pain, especially when the pain is mild and confined to a specific area. These treatments are often introduced early in a care plan or paired with systemic therapies to improve pain management.
One of their key advantages is the ability to offer focused relief while reducing the risk of side effects that can come with medications affecting the whole body. However, it’s important to consult a healthcare professional to figure out the most suitable option for your individual situation.
Related Blog Posts
- Neurostimulation: Future of Dental Pain Relief
- Studies on Pain Management in Dental Extractions
- Antidepressants in Orofacial Pain: Evidence Summary
- How Combination Analgesics Manage Orofacial Pain
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





