







Adjunctive Therapies for Pain in Paediatric Dentistry

Managing pain and anxiety in paediatric dentistry is challenging but crucial for creating positive dental experiences for children. Pain, even minor, can lead to long-term dental fear and avoidance. This article explores effective adjunctive therapies – both pharmacological and non-pharmacological – used alongside local anaesthesia to ease discomfort during procedures.
Key Takeaways:
- Non-Pharmacological Methods: Techniques like Transcutaneous Electrical Nerve Stimulation (TENS), vibrotactile devices, and audiovisual distractions (e.g., cartoons, VR) significantly reduce pain and anxiety. Studies show VR can cut pain perception by 50% and anxiety by 53%.
- Pharmacological Approaches: Options include topical anaesthetics (e.g., lidocaine), preoperative pain relievers (e.g., ibuprofen), and advanced delivery systems like computer-controlled local anaesthesia. Articaine has shown better pain relief than lidocaine in children.
- Audiovisual Distraction: Combining sight and sound (e.g., cartoons, gaming consoles) reduces pain scores and stress indicators. For example, PlayStation use during treatment dropped pain scores from 8.5 to 2.3.
- Virtual Reality: Immersive VR distracts the brain from pain signals and reduces stress. However, practical challenges include headset weight, hygiene concerns, and potential side effects like nausea.
- Pain-Triggering Tools: Dental drills, needles, and extraction tools are major sources of discomfort. Techniques like vibrotactile devices and distraction can make these less distressing.
Combining these methods – physical counter-stimulation, cognitive distraction, and targeted medications – offers the most effective approach to managing pain and anxiety in children. However, standardising pain assessment tools and improving practitioner training remain key challenges.
New guidelines for pain control: Pediatric dental patients
sbb-itb-2be92ed
Audiovisual Distraction Techniques
Audiovisual distraction combines sight and sound to draw focus away from dental procedures. Research shows this method works far better than audio-only distractions or traditional behaviour management strategies like "tell-show-do" [6][8].
The audio component plays a critical role – mute-video distraction has little to no effect during procedures like anaesthetic injections [7]. When children experience both visual and auditory immersion, such as through headphones paired with engaging content, the sensory experience helps mask clinical sounds and reduces their awareness of what’s happening. This makes it an excellent complement to pharmacological methods discussed later.
"Mute‐video distraction has no significant efficacy for reduction of pain and anxiety… Audiovisual distraction, however, can effectively decrease the pain and anxiety of paediatric dental patients during anaesthetic injection." – Dental Research Journal [7]
Pain Reduction Results
Clinical studies back up the effectiveness of audiovisual tools in reducing pain. A 2019 study at Indira Gandhi Government Dental College tested 60 children aged 5–9 undergoing pulp therapy, dividing them into three groups: one using a PlayStation gaming console, one reading comic books, and a control group. The PlayStation group showed a dramatic drop in pain scores, averaging 2.3 on the Wong-Baker Faces Scale compared to 8.5 in the control group – a statistically significant result (p < 0.001) [8].
Beyond pain scores, this method also lowers stress indicators and helps parents perceive their child as less anxious. For instance, a study of 60 children aged 4–7 revealed audiovisual distraction significantly reduced pulse rate spikes during local anaesthetic injections. Parents rated their child’s anxiety at 7.75 in the audiovisual group, compared to 18 in the control group [7][8]. Meta-analyses suggest pain reduction during procedures can reach highly significant levels (p < 0.00001) [5]. This approach is especially effective for children aged 3–8, who are old enough to engage with media but still highly responsive to sensory distractions [5].
Setting Up Audiovisual Tools in Clinics
Introducing this technique in clinics involves choosing and configuring the right equipment. Popular options include video eyeglasses (like VESS systems or "Cool Vision 3"), gaming consoles such as PlayStation, or screens mounted to dental units or positioned within the child’s line of sight [5][8]. These tools allow for flexibility based on the clinic’s setup and patient needs.
Between June and October 2022, Istanbul Medipol University trialled a cartoon-assisted distraction system with 68 children aged 4–9. A screen attached to the dental unit displayed one of 12 pre-approved films chosen by the child. Led by researcher N. Ugurlu, the study found that while this setup didn’t significantly lower anxiety during anaesthetic injections, it did reduce self-reported pain during treatment (p < 0.025) [10].
To maximise effectiveness, volume should be high enough to mask unpleasant sounds like drills but still allow the child to hear instructions. Introducing the device a few minutes before the procedure helps the child settle into the content [8][9][10][11]. Allowing children to pick what they watch also gives them a sense of control, which can ease anticipatory stress [10].
In September 2024, the University of Salerno introduced the "UNISA-Virtual Stepwise Distraction model" designed for children with Special Healthcare Needs. This method spans three visits: starting with audiovisual projection for familiarisation, moving to AV glasses for desensitisation, and culminating in using AV glasses during restorative treatment to block out drill sounds [11].
Virtual Reality for Pain Management
Virtual reality (VR) goes beyond simple distraction techniques by immersing children in a fully sensory experience. The way it works is fascinating – VR occupies the brain’s limited attention span, leaving fewer resources to process pain signals. Brain imaging studies show that VR use during painful events can cut activity in the "pain matrix" areas of the brain – like the anterior cingulate cortex, insular cortex, and thalamus – by over 50% [12][13].
The technology also helps by blocking visual and auditory triggers. For example, VR headsets shield children from seeing needles or sharp tools, while headphones drown out unsettling sounds like dental drills [12][14]. This combination creates a sense of "presence", where kids feel like they’ve been transported to another world, making it easier for them to relax [13][15].
"The brain is so pre-occupied with processing information presented via virtual reality, that the patient has less attention available to process incoming pain signals." – Hunter G. Hoffman, University of Washington [13]
Clinical Research on VR
Recent studies highlight how effective VR can be in managing pain for children. For instance, a randomised controlled trial conducted at the Jordan University of Science and Technology (June 2023–August 2024) tested the Vuzix iWear VR goggles on 154 children aged 5–12. The results? VR halved pain perception during procedures like extractions and pulp therapy, boosting patient relaxation to 70.31%, regardless of whether local anaesthesia was used [14].
A 2024 meta-analysis backed these findings, showing that immersive VR significantly reduced pain intensity (SMD = -0.99) and anxiety (SMD = -0.53) in paediatric patients [12]. In another study with the Oculus Rift, kids reported a 42% drop in "worst pain" and a 75% drop in "pain unpleasantness" compared to standard care [13]. Beyond pain relief, VR also lowered heart rate (SMD = -0.91) and electrodermal activity, indicating reduced stress during procedures [12][15]. And it wasn’t just about reducing discomfort – VR made dental visits more enjoyable, increasing the "fun" factor by 61% [13].
The type of content matters too. Non-violent, calming visuals like underwater scenes or animated shows such as SpongeBob SquarePants work best for relaxation [14][15]. A study conducted between September and November 2024 in Timișoara, Romania, observed 120 children aged 6–12 using the Kit Limbix VR system during non-invasive procedures like fluoride treatments. By monitoring stress via E4 biometric wristbands, researchers recorded noticeable reductions in heart rate and perspiration when kids were immersed in nature scenes or cartoons [15].
Limitations and Practical Considerations
While VR shows great promise, it’s not without challenges. Most headsets weigh about 700 grams, which can feel heavy for younger children. Their bulk can also interfere with a dentist’s ability to access the mouth, especially when the child is lying down in a dental chair [12][16].
Hygiene is another concern. Clinics need to use single-use covers or thoroughly disinfect headsets between patients to maintain cleanliness [12]. Additionally, some children experience "cyberkinetosis" – symptoms like nausea, dizziness, or sweating – within minutes of using VR [12]. It’s also not suitable for kids with epilepsy, severe vestibular issues, or certain developmental delays [12][14].
Letting children try the headset in the waiting room can help them adjust to the technology and avoid being overwhelmed during the procedure [12]. Some dentists prefer "mini" VR glasses over full-sized headsets, as they cover less of the face and make kids feel less isolated [16]. While the initial cost of VR equipment and training can be high, many clinics find the improved cooperation and reduced need for sedatives make it a worthwhile investment [12][14].
Pharmacological Pain Management Options
While non-pharmacological methods like audiovisual and virtual reality techniques help distract young patients, pharmacological approaches directly target the pain itself, making them an essential part of paediatric dentistry. Local anaesthetics are the cornerstone of pain management in this field, and advancements in their delivery and formulation have greatly improved both their safety and effectiveness.
A noteworthy study conducted at the Dentistry Clinic of Vojvodina (January–April 2022) compared two common anaesthetics in 60 patients aged 5–18. Researchers tested 1.7 mL of 4% articaine (via buccal infiltration) against 1.8 mL of 2% lidocaine (via inferior alveolar nerve block). The results showed that articaine produced a mean Wong-Baker pain score of 1.33, compared to 3.17 with lidocaine [20]. These findings highlight that articaine administered through buccal infiltration can offer superior pain relief for invasive dental procedures in children.
Lidocaine Infusions for Acute Pain
When children experience severe or persistent pain – especially following major dental procedures under general anaesthesia – continuous intravenous lidocaine infusions can be a highly effective option. These infusions provide central pain relief while reducing the need for opioids. A review conducted in May 2021 by researchers at the University of Tennessee Health Science Center examined 51 lidocaine infusions administered to 29 paediatric patients (median age 14). The standard protocol involved a 1.5 mg/kg bolus over 30 minutes, followed by a maintenance dose of 1 mg/kg/h. The results showed significantly lower pain scores (p < 0.001) and reduced reliance on opioids [19].
"Lidocaine is inexpensive and carries minimal risk of serious side effects due to its short plasma half-life." – Elizabeth A. Hall, PharmD, University of Tennessee Health Science Center [19]
Safety is paramount when using lidocaine infusions. Continuous ECG and neurological monitoring are essential. In the Tennessee study, 24% of infusions resulted in mild side effects like upper extremity paraesthesia (10%) and visual disturbances (4%), all of which resolved after dose adjustments or stopping the infusion [19]. To ensure safety, serum concentrations should be maintained between 2–5 mcg/mL.
Additional Pharmacological Methods
Advances in technology and technique have introduced new ways to enhance pain management. For example, computer-controlled local anaesthesia delivery (CCLAD) systems, such as ‘The Wand‘, provide a steady flow rate, reducing tissue resistance and making injections less uncomfortable [18].
Another improvement is buffering local anaesthetic cartridges with 8.4% sodium bicarbonate at the chairside. This approach speeds up the onset of anaesthesia and reduces injection discomfort [18].
To address the issue of prolonged numbness, which can lead to accidental lip or cheek biting, phentolamine mesylate (Oraverse) can be used. This agent reduces the duration of numbness in children (ages 4–11) from 135 minutes to about 60 minutes [18]. However, weight-based dosing is critical to ensure safety. Clinicians must calculate the maximum safe dose (mg/kg) for each child, factoring in all anaesthetic agents used, including topicals, to avoid toxicity [18][21].
Discomfort from Dental Tools and Procedures
Even with local anaesthesia, dental instruments can still cause a fair amount of discomfort. Understanding which tools are most distressing allows clinicians to adjust their methods and monitor pain levels to reduce patient discomfort. Below, we’ll explore the tools that tend to cause the most discomfort and some practical strategies to ease these effects.
Tools That Cause Discomfort
Extraction tools top the list for causing discomfort, with an average pain score of 46.51 mm on the Visual Analogue Scale (VAS). This is largely due to the tissue trauma caused by the pressure and force needed during extractions [22][24]. Not far behind are dental drills, which score an average of 41.83 mm. The combination of high-speed rotation, loud noise, and vibrations makes drills particularly unsettling for many patients [22][23].
"The sight, sensation, and fear of pain from the needle and dental drill have been frequently reported to be the most fear-evoking stimuli for dentally anxious children." – Pesqui. Bras. Odontopediatria Clín. Integr. [23]
Syringes and needles are another major source of discomfort, with a mean VAS score of 36.04 mm. They not only cause physical pain but also psychological distress, especially in children. More than half of paediatric dentists identify them as a key trigger for fear [22][24]. Even less invasive tools like suction devices and handpieces can cause distress due to their noise, while rubber dams often feel uncomfortable because of the pressure and restrictive sensation they create during placement [24].
Reducing Tool-Related Pain
Minimising discomfort from dental tools requires a thoughtful, step-by-step approach. One effective strategy is stepwise procedure planning. This involves starting with simpler, less invasive tools, such as polishing instruments, which have a much lower VAS score of 22.28 mm, and gradually moving to more complex ones. This approach not only builds trust but also helps desensitise patients to the process [22][23].
Managing noise is another key factor. Using audiovisual distractions like 3D VR glasses and headphones can help mask the unsettling sounds of air rotors and suction devices [4]. For needles, vibrotactile devices such as DentalVibe or Vibraject offer a clever solution. These tools use vibrations to disrupt pain signals, in line with the Gate Control Theory. A 2024 study with 150 children aged 8–12 showed that DentalVibe reduced pain to an average score of just 1.68 on a 10-point scale, compared to 9.2 for standard needle techniques [25].
Keeping sharp tools out of sight is another simple but effective method. Shielding syringes from a child’s view can prevent anticipatory anxiety [24]. The "Tell-Show-Do" technique is also highly effective: explaining tools in simple, friendly terms before using them helps ease fears and encourages cooperation [23][24]. When combined with distraction techniques and pharmacological aids, these methods create a well-rounded approach to managing pain and anxiety in paediatric dental care.
Comparing Pain Management Therapies
Comparison of Pain Management Therapies in Paediatric Dentistry
Choosing the right pain management method means weighing the strengths and drawbacks of each option. Non-pharmacological approaches, like virtual reality (VR) and audiovisual distractions, are particularly effective for easing pain-related anxiety during short, acute procedures – think dental injections [17] [27]. On the other hand, pharmacological options such as NSAIDs and paracetamol are more suited for managing postoperative pain, especially after procedures involving general anaesthesia. Among these, preoperative NSAIDs have shown better results compared to paracetamol alone [28].
Immersive distraction methods, such as VR, have been shown to outperform simpler alternatives. For instance, a clinical trial conducted in 2025 revealed that children using VR headsets during dental injections experienced significantly less anxiety and pain during inferior alveolar nerve blocks (IANB). BMC Pediatrics [17] noted:
"Using a VR headset significantly decreased anxiety and pain during the IANB, while using headphones had no particular advantage."
Similarly, vibrotactile devices, especially when combined with cold applications, have proven to be more effective than standard injection techniques. Research involving 1,094 paediatric patients highlighted consistent pain reduction with these methods [2].
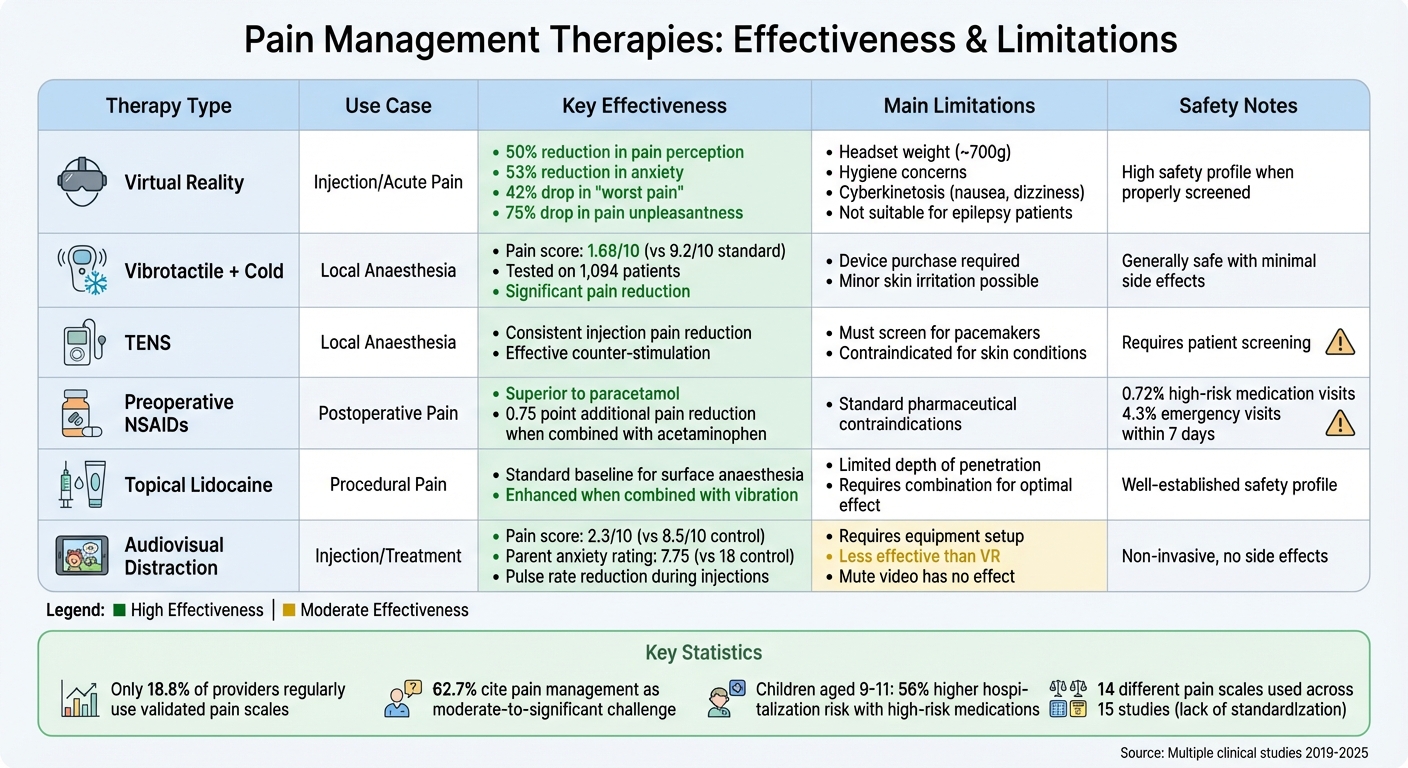
To make informed decisions, it’s essential to consider the safety and practicality of each method. Below is a summary of key therapies and their characteristics:
| Therapy Type | Use Case | Key Effectiveness | Main Limitations |
|---|---|---|---|
| Virtual Reality | Injection/Acute Pain | High reduction in pain/anxiety [17] | Physical discomfort from headset; technical setup [17] |
| Vibrotactile + Cold | Local Anaesthesia | Significant reduction in pain scores [26] | Requires device purchase; minor skin irritation possible [2] |
| TENS | Local Anaesthesia | Consistently reduces injection pain [2] | Must screen for pacemakers/skin conditions [4] |
| Preoperative NSAIDs | Postoperative Pain | Superior to paracetamol for post-extraction pain [28] | Standard pharmaceutical contraindications apply |
| Topical Lidocaine | Procedural Pain | Standard baseline for surface anaesthesia [2] | Effectiveness enhanced when combined with vibration [2] |
Pharmacological safety is a key concern, particularly in paediatric care. Around 0.72% of children’s dental visits involve high-risk medications like opioids or benzodiazepines, with 4.3% resulting in emergency visits within seven days [29] [30]. Alarmingly, children aged 9 to 11 face a 56% higher likelihood of hospitalisation after receiving such medications compared to adolescents [30]. This highlights the importance of prioritising non-opioid strategies and integrating non-pharmacological techniques.
Blending different approaches often leads to better outcomes. For example, combining physical counter-stimulation methods (like vibration and cold) with cognitive distractions (such as VR) addresses both the physical and emotional aspects of pain [26]. For Australian clinics participating in the Child Dental Benefits Scheme – which offers up to AU$1,000 per eligible child over two years – these evidence-based methods provide an affordable and effective way to improve care while minimising reliance on high-risk medications.
Conclusion
Managing pain effectively in paediatric dentistry calls for a dual focus on reducing both pain and anxiety. Beyond the previously explored benefits of virtual reality (VR) and vibrotactile devices, combining medications like acetaminophen and ibuprofen with distraction techniques has proven to enhance pain relief. For example, pairing acetaminophen (15 mg/kg) with ibuprofen (5 mg/kg) can lower pain intensity by an additional 0.75 points on a four-point scale compared to acetaminophen alone [31]. However, the lack of consistent research limits the creation of universal guidelines.
One major hurdle is the inconsistency in pain assessment methods. A systematic review found 14 different pain scales used across just 15 studies, making it tough to compare findings or establish standard practices [3]. Emily Xin Yi Ting from Adelaide Dental School highlights this issue:
"This review underscores the challenges in reliably assessing pain in children and highlights the necessity for age-specific validated pain assessment tools." [3]
Small sample sizes and ethical constraints further complicate research, leaving many common therapies without high-certainty evidence [1][33]. These gaps emphasise the importance of standardising pain assessment tools to improve both research and clinical outcomes. For more clinical insights, visit our dental blog.
In practice, challenges persist. Only 18.8% of paediatric dental providers regularly use validated pain scales, while 62.7% cite pain management as a moderate to significant challenge in their work [32]. Barriers such as time limitations, insufficient training, and inconsistent insurance coverage make it harder for practitioners to adopt these methods. Overcoming these obstacles will require better training, accessible family education resources, and tools to mitigate anxiety transfer from parents to children.
Looking ahead, future research must focus on large-scale, rigorous clinical trials with clear protocols and age-specific assessment methods. Therapies like Low-Level Laser Therapy need standardised application guidelines, while pharmacological combinations require more robust safety data [2][31]. In Australia, incorporating these evidence-based strategies into systems like the Child Dental Benefits Scheme could enhance care quality while reducing reliance on high-risk medications. The combination of physical counter-stimulation, cognitive distraction, and targeted analgesics represents the current gold standard for managing paediatric dental pain [26].
FAQs
Which pain-control option is best for my child’s age and procedure?
The right way to manage your child’s pain depends on their age, the type of procedure, and their unique needs. For many treatments, like extractions, pharmacological options such as local anaesthetics are commonly used. On the other hand, non-pharmacological methods, like distraction techniques or reducing anxiety, can work well as additional support. Often, a mix of both approaches gives the best results. It’s important to talk to your child’s dentist to figure out the most suitable pain management plan based on the latest evidence and recommendations.
Is VR safe for kids, and who shouldn’t use it?
Virtual reality (VR) is often regarded as a safe option for children and has proven effective in reducing pain and anxiety during paediatric dental treatments. That said, it’s not ideal for every child. Kids with epilepsy, visual or balance-related impairments, or those who experience motion sickness may not be suitable candidates for VR. It’s crucial to have professional supervision and carefully assess each child’s medical history and tolerance before considering VR as a tool for managing pain.
What can parents do before the visit to reduce dental anxiety?
Parents play a key role in helping children feel more at ease during dental visits. Techniques like modelling, where parents or siblings demonstrate calm behaviour during dental procedures, can set a positive example. Positive reinforcement, such as praising or rewarding children after a visit, encourages a sense of accomplishment. Using audiovisual distractions like cartoons or music can shift their focus away from the procedure, while relaxation methods – like deep breathing exercises – help reduce tension. These approaches can make dental appointments less stressful and more comfortable for kids.
Related Blog Posts
- Acupuncture vs. Relaxation: Pain Relief in Dentistry
- Advances in Orthodontic Pain Management Techniques
- Comparing Pain Relief Methods for Kids: What Works Best?
- How Dentists Manage Pain for Different Age Groups
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





