







How Dentists Manage Pain for Different Age Groups

Dentists use different pain management strategies depending on a child’s age and developmental stage. From infants to adolescents, methods include tailored medication dosages, behavioural techniques, and specialised tools to assess and address discomfort. Here’s a quick look:
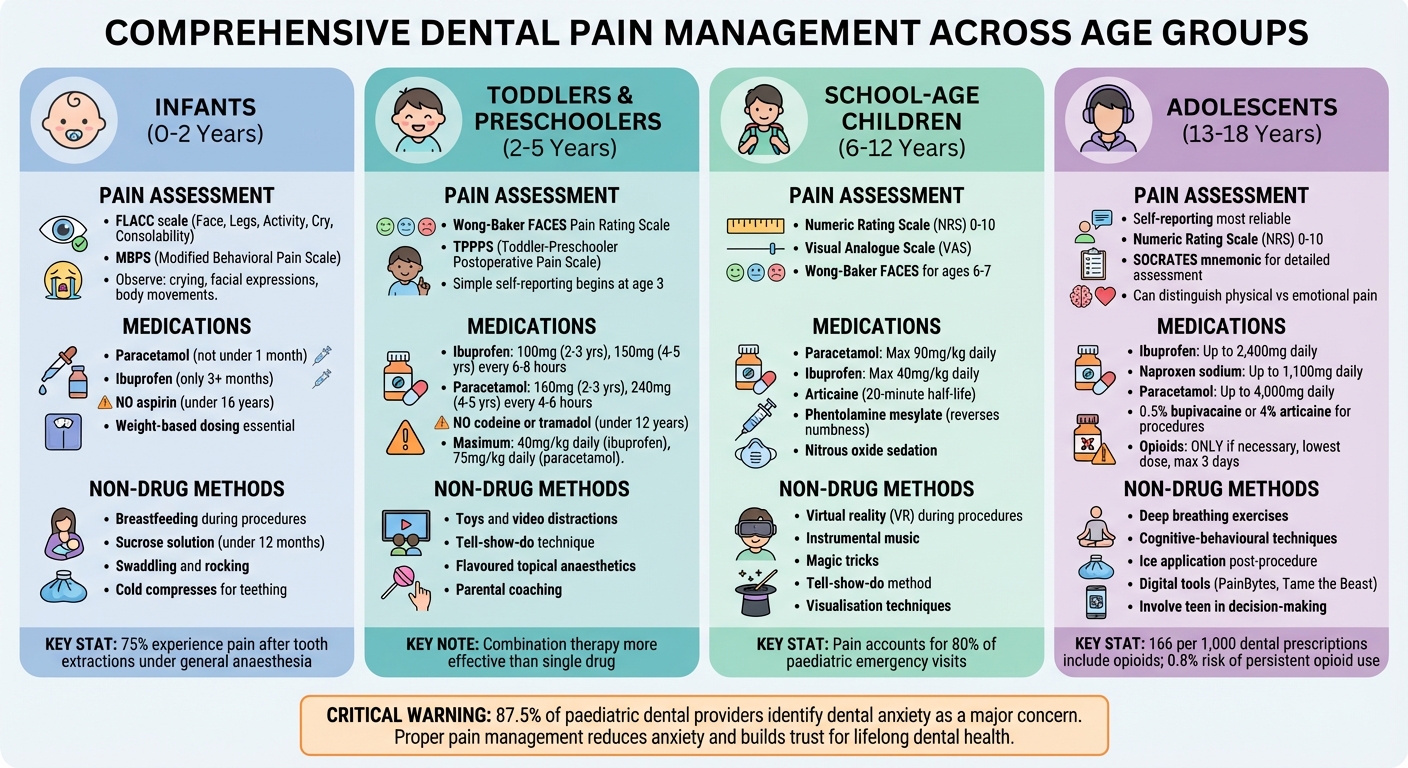
- Infants (0–2 years): Pain is assessed through behaviours like crying or grimacing. Common strategies include paracetamol, ibuprofen, breastfeeding during procedures, or sucrose solutions for short-term relief.
- Toddlers & Preschoolers (2–5 years): Simple self-reporting begins, supported by tools like the Wong-Baker FACES scale. Distraction, local anaesthetics, and age-appropriate medication are key.
- School-Age Children (6–12 years): They can use numeric pain scales and benefit from distractions like virtual reality. Medications like ibuprofen and paracetamol are used with precise dosing.
- Adolescents (13–18 years): Self-reports are reliable. Pain management includes NSAIDs, local anaesthetics, and psychological techniques like breathing exercises. Opioids are used sparingly due to risks of dependency.
Each approach ensures safe and effective care, reducing anxiety and building trust in dental visits.
Age-Specific Dental Pain Management Strategies for Children
1. Infants (0-2 Years)
Pain Assessment Tools
Since infants can’t verbalise their pain, assessing it relies entirely on observation. Healthcare professionals use behavioural scales that focus on facial expressions, body movements, and crying patterns. One widely used tool is the FLACC scale (Face, Legs, Activity, Cry, Consolability), which scores each category from 0 to 2 and is suitable for infants as young as two months [3][4]. Other tools include the MBPS (Modified Behavioral Pain Scale) for procedural pain, such as injections, and COMFORT-B for monitoring pain in intensive care settings [3][4].
A major challenge is differentiating pain from other discomforts like hunger or fear. As BMC Pediatrics highlights:
The problem of differentiating or discriminating pain from other expressions of unpleasant feelings or experiences, such as hunger, fear or distress adds to the complexity of assessing pain in this group [3].
Physical signs, such as changes in skin colour, sweating, pallor, or shifts in heart rate and oxygen levels, also play a role in identifying pain [1]. These observations help guide decisions about appropriate pain relief methods.
Pharmacological Strategies
For mild to moderate dental pain, paracetamol and ibuprofen are the most commonly used medications [6][1]. Dosages must always be determined by the infant’s weight, using the provided measuring device for accuracy [1]. Paracetamol is not recommended for infants under one month, and ibuprofen should only be used for those older than three months [1]. Aspirin is strictly prohibited for children under 16 due to the risk of Reye’s syndrome [1].
In dental procedures, local anaesthetics like lignocaine or articaine are employed to numb the area through infiltration or topical application [2]. For more complex treatments requiring general anaesthesia, medications such as IV paracetamol, fentanyl, or rectal suppositories may be used [2]. Studies suggest that combining paracetamol and ibuprofen is often more effective than using either drug on its own [6].
Non-pharmacological approaches can further improve comfort, making them a valuable complement to medications.
Non-Pharmacological Techniques
Simple comfort measures can make a significant difference in reducing an infant’s distress. Breastfeeding during procedures is highly effective for babies under six months [1]. For infants under 12 months, a sucrose solution can help ease pain during short procedures [1]. Non-nutritive sucking, such as using a pacifier, has also been shown to reduce neonatal pain (SMD -1.20) [5]. Techniques like swaddling, rocking, or holding are equally beneficial, with rocking demonstrating an SMD of -0.75 for immediate pain relief [5].
For dental discomfort, cold compresses and teething rings can provide relief [7][1]. As infants near two years old, distractions like toys or books become effective tools for soothing [5][1]. However, topical benzocaine products should be avoided for teething pain in children under two years due to the risk of methaemoglobinaemia [7].
Developmental Considerations
Research confirms that infants have the capacity to feel and respond to pain from birth [5]. However, since they can’t communicate verbally, caregivers must look for behavioural changes such as irritability, reduced appetite, or unusual quietness [5][1]. General anaesthesia is often necessary during dental treatments, as infants cannot cooperate in a standard dental chair [2]. Postoperative pain is common, with around 75% of children experiencing discomfort after primary tooth extractions under general anaesthesia [2]. This makes early and effective pain management crucial.
These tailored approaches for infants lay the groundwork for the broader age-specific strategies explored throughout the article.
sbb-itb-2be92ed
2. Toddlers and Preschoolers (2-5 Years)
Pain Assessment Tools
When assessing pain in toddlers and preschoolers, the approach evolves to include early self-reporting alongside observational methods. For children aged 2–3, verbal communication about pain is still underdeveloped, so behavioural cues like facial expressions, crying, and limb movements remain the most dependable indicators [8][9][10]. Tools like the Toddler-Preschooler Postoperative Pain Scale (TPPPS), which observes pain-related behaviours over a 5-minute period, are particularly effective for children aged 1–5 years [9][10]. The FLACC scale, already used for infants, continues to be valuable for children up to 7 years old [10].
By age 3, children begin to distinguish pain severity using simple scales, such as "no pain, little pain, a lot" [9][10]. The Wong-Baker FACES Pain Rating Scale becomes an excellent tool at this stage. As Priya Nagarwal explains:
Out of all the scales discussed, Wong-Bakers facial pain rating scale (WB-FPS) is considered the best as it is simple to use for the operator and can be easily reproduced and can be used in children as young as 3 years of age [8].
By 4–5 years, most children can use more detailed pain scales with 4–5 levels and provide better ratings of pain intensity [9][10]. For facial scales, the Revised Faces Pain Scale (FPS-R) is preferred, as versions with smiling faces can confuse emotional expression with actual pain [10]. These tools ensure accurate pain assessment, which directly informs age-specific treatment strategies.
Pharmacological Strategies
For toddlers and preschoolers, nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen are the first choice for managing acute dental pain [7]. Correct weight-based dosing is crucial to avoid risks like liver damage from paracetamol or stomach issues from NSAIDs [7][1]. Dosages for acute dental pain are as follows:
- Ibuprofen: 100 mg every 6–8 hours for 2–3 year olds, 150 mg for 4–5 year olds (maximum 40 mg/kg daily)
- Paracetamol: 160 mg every 4–6 hours for 2–3 year olds, 240 mg for 4–5 year olds (maximum 75 mg/kg daily) [7]
A combination of NSAIDs and paracetamol is often more effective than either alone [7][6]. Importantly, opioids like codeine and tramadol are strictly prohibited for children under 12 due to severe risks, including respiratory depression [7]. Long-acting local anaesthetics, such as bupivacaine, are also avoided in young children to minimise the risk of soft tissue injuries while numbness persists [7][2]. Always use the provided dosing device for accuracy – never rely on a kitchen spoon [1].
Non-Pharmacological Techniques
Non-drug approaches for managing pain in this age group focus on cognitive and behavioural techniques. Toddlers respond well to physical comfort and simple distractions like toys, while preschoolers benefit from more interactive distractions, such as videos or video glasses during procedures [11][1]. Allowing preschoolers to make small choices, like picking a medicine flavour, can also help reduce anxiety.
Parental involvement becomes more targeted at this stage. Parents can be coached to use specific techniques like shushing, rubbing, or distraction. Avoid misleading reassurance – don’t tell a child a procedure won’t hurt if it will. Instead, use clear, simple language to explain what’s happening, which helps reduce fear [1]. For dental treatments, strategies like needle desensitisation and flavoured topical anaesthetics can make local anaesthesia more acceptable to children [11].
Developmental Considerations
Pain management in toddlers and preschoolers must account for their developmental stage. By age 2, children can often point to where it hurts but may struggle to describe the intensity [9][10]. Toddlers often express pain through "regression" behaviours like thumb sucking, loss of appetite, or becoming unusually quiet [1]. Preschoolers, on the other hand, can start to articulate their discomfort more effectively.
Fear and anxiety significantly amplify pain perception in this age group. Creating a calm environment and communicating clearly are key to easing situational stress [1][10]. The goal isn’t necessarily to eliminate pain entirely but to make it manageable for the child [7][1].
3. School-Age Children (6-12 Years)
Pain Assessment Tools
By the time children reach school age, they can often self-report pain using numerical scales. Kids aged 8 and above tend to handle tools like the Numeric Rating Scale (NRS) or Visual Analogue Scale (VAS) well, rating their pain on a 0–10 scale. For younger kids in this range (ages 6–7), pictorial tools like the Wong-Baker FACES® or FPS-R are more effective, as abstract reasoning is still developing. However, some children might downplay their pain to seem "brave", so clinicians should always pair these self-reports with careful observation of behavioural signs [12]. Pain accounts for up to 80% of visits to paediatric emergency departments, making accurate assessment crucial [12]. These evaluations directly guide the choice of appropriate treatments.
Pharmacological Strategies
Accurate dosing is critical when treating pain in school-age children. As with younger age groups, weight-based dosing is essential to avoid overdoses. For instance:
- Paracetamol: Maximum daily dose is 90 mg/kg.
- Ibuprofen: Should not exceed 40 mg/kg daily [14].
For acute musculoskeletal pain or migraines, ibuprofen often works faster and more effectively than paracetamol [12]. On the other hand, aspirin is strictly avoided due to the risk of Reye syndrome, and opioids like codeine are rarely used because of the potential for respiratory depression [14].
Local anaesthetics also require weight-based calculations. Articaine, a commonly used dental anaesthetic, has a short half-life of just 20 minutes, reducing systemic exposure [13]. For children 6 and older, phentolamine mesylate can help reverse numbness faster, preventing accidental injuries like lip-biting after dental work [14]. Additionally, school-age children are generally more comfortable using nitrous oxide sedation, as they can wear a nasal hood and follow instructions without difficulty [14].
Non-Pharmacological Techniques
Distraction techniques are particularly effective for this age group, thanks to their developing cognitive skills. For example, virtual reality (VR) has shown significant success in reducing pain during dental procedures in children aged 5–12 [13]. Other useful distractions include:
- Instrumental music
- Magic tricks
- Active movement-based activities [16]
The "tell-show-do" method, which involves explaining, demonstrating, and then performing a procedure, is widely used. Paired with supportive language and positive reinforcement, it helps children feel more at ease [17].
Preparing children mentally is just as important. Stories about dental visits or informational pamphlets can help them build coping skills and reduce anxiety [16]. Techniques tailored to their intellectual level – like visualisation or persuasion – can make a big difference. As research has shown, lowering dental anxiety can significantly increase a child’s pain tolerance [13].
Developmental Considerations
Developmental factors also play a big role in shaping pain management strategies. For instance, the mandibular foramen in children is located closer to the occlusal plane than in adults, necessitating adjusted injection techniques for effective nerve blocks [14]. Anxiety and fear can amplify pain perception by activating the pituitary-adrenal axis, making proper anxiety management crucial [12].
Failing to treat acute pain adequately during childhood can have long-term consequences, potentially altering brain structure and affecting cognitive and emotional health into adulthood [12]. Using age-appropriate language – like calling an ultrasonic scaler "Mr. Whistle" – can also help kids feel less anxious, improving their overall experience [14].
Parents are key players in post-operative care, with 87.4% of providers emphasising their importance in managing pain after procedures [17]. By tailoring strategies to developmental stages, clinicians can significantly improve outcomes, ensuring children receive the care they need in a way that supports both their immediate and long-term well-being.
4. Adolescents (13-18 Years)
Pain Assessment Tools
Adolescents are typically reliable when it comes to self-reporting pain, making this the most accurate way to assess their discomfort. The Numeric Rating Scale (NRS) is a common tool used for this age group, where teens rate their pain from 0 (no pain) to 10 (worst pain imaginable). They can also distinguish between physical pain and emotional distress, as well as describe the type and location of their pain – whether it’s aching, burning, or stabbing [18].
"All professionals agree that a teen’s self-report of pain takes priority over observation by others. In other words, even if a teen can laugh or sleep or otherwise does not look like they are in pain, if they say they are in pain it must be taken seriously." – SickKids Staff [18]
In addition to self-reports, clinicians should watch for behavioural signs like irritability, sudden mood swings, difficulty moving, and withdrawal from social activities. For adolescents with developmental or intellectual disabilities who cannot self-report, tools such as the Non-Communicating Children’s Pain Checklist (NCCPC) are useful. Comprehensive assessments might also include the SOCRATES mnemonic (Site, Onset, Character, Radiation, Association, Time course, Exacerbating/Relieving factors, and Severity) to gather a detailed understanding of the pain [6].
Pharmacological Strategies
For acute dental pain, NSAIDs like ibuprofen (up to 2,400 mg daily) or naproxen sodium (up to 1,100 mg daily) are the first-line treatment and can be combined with paracetamol (up to 4,000 mg daily) for added relief [15]. After surgical procedures, such as extractions, long-acting local anaesthetics like 0.5% bupivacaine or 4% articaine may provide longer-lasting pain control compared to lignocaine [15].
However, opioid use in this age group is a serious concern. In 2015, 166 out of every 1,000 dental prescriptions for adolescents aged 11 to 18 years included an opioid. Alarmingly, teens prescribed opioids after third-molar extractions face a 0.8% higher risk of developing persistent opioid use and a 1.6% higher risk of substance use disorders. Even a single exposure can increase the likelihood of opioid addiction in this group [15].
When opioids are absolutely necessary, they should be prescribed at the lowest effective dose for no more than three days. Clinicians must review the patient’s medical and social history, check for any recreational drug use, and consult the state’s prescription drug monitoring program before prescribing. It’s also crucial to set realistic expectations, advising teens that some level of manageable pain is normal rather than aiming for complete pain relief [15].
Non-Pharmacological Techniques
A team-based approach works best, involving the adolescent in planning their pain management alongside parents and dentists. This not only respects their growing need for independence but also encourages better adherence to the treatment plan [20]. Simple physical interventions, like applying ice to the jaw after procedures such as wisdom teeth removal, can help reduce swelling and pain.
"Involving adolescents in the pain management decision-making process and allowing them to carry out the plan with some caregiver support was acceptable and well executed following third molar extractions." – BMC Pediatrics [20]
Other strategies include psychological techniques such as deep breathing exercises and cognitive-behavioural methods to address dental anxiety – a challenge reported by 87.5% of paediatric dental providers [17]. Digital tools like PainBytes and Tame the Beast can also help teens better understand pain and shift their perspective on it. These approaches are tailored to balance guidance with the teen’s desire for autonomy [17].
Developmental Considerations
Adolescents vary widely in how they perceive and respond to pain due to differences in cognitive and emotional development [19]. Factors like gender and societal expectations can also play a role – boys may downplay their pain to avoid appearing vulnerable, while girls might be more open about their discomfort. Some teens may even hide their pain to appear as "good patients" and avoid disappointing their healthcare providers [18].
The role of parents evolves during treatment. While only 13.7% of providers see parental presence as essential during procedures – since many teens prefer privacy – 87.4% consider parental support critical afterward. Tasks like reminding teens to take medication or apply ice often fall to parents [17][20]. Dentists are encouraged to communicate directly with adolescents about their pain while remaining aware of the information they might be gathering from peers or social media [20].
How to Manage Children in Dental Pain – Paediatric Emergencies – PDP159
Advantages and Limitations
When managing pain in paediatric patients, balancing effectiveness and safety is a top priority. Each treatment option has its own pros and cons, which can vary depending on the child’s age and specific needs.
Paracetamol is widely regarded as a safe first-line option. Approved for use from one month of age [21][22], it works by increasing pain tolerance through the central nervous system. However, its lack of anti-inflammatory properties and the risk of liver damage from overdosing – typically at doses over 150 mg/kg – are important considerations [21].
NSAIDs like ibuprofen are particularly effective for managing inflammatory dental pain. Ibuprofen is approved for children as young as three months, while naproxen is only recommended for those over two years old [21][7]. Despite their benefits, NSAIDs come with risks such as gastrointestinal bleeding and renal issues, particularly in children who are dehydrated or have underlying health conditions [21][22]. Additionally, about 2% of children with asthma may have a sensitivity to ibuprofen [21].
"Taking ibuprofen and paracetamol together has been recommended because the combination is more effective than either drug alone." – Aovana Timmerman, Specialist Endodontist [6]
Behavioural techniques – like distraction, "tell-show-do", and deep breathing – are non-pharmacological methods that help manage dental anxiety without medication. Dental anxiety is a significant issue, with 87.5% of paediatric dental providers identifying it as a major or moderate concern [17]. While most providers (73.2%) believe the typical 5–10 minutes spent on pain management is sufficient, behavioural strategies are best used alongside medication rather than as a standalone solution [7].
The table below highlights the main advantages and limitations of each approach:
| Approach | Primary Advantage | Primary Limitation | Best For |
|---|---|---|---|
| Paracetamol | High safety profile; fewer adverse effects [21] | Lacks anti-inflammatory effect; risk of liver toxicity [21] | Mild to moderate pain, headaches, minor post-operative discomfort [21] |
| NSAIDs (Ibuprofen/Naproxen) | Effective for inflammatory and dental pain [21][6] | Risk of gastrointestinal bleeding and renal impairment [21][22] | Dental pain, musculoskeletal injuries, inflammatory conditions [21][7] |
| Combination Therapy | Provides effective non-opioid pain relief [6][7] | Requires strict adherence to two dosing schedules [6][7] | Post-extraction pain, moderate to severe dental discomfort [6][7] |
| Behavioural Techniques | Reduces anxiety and improves long-term dental attitudes [17] | Does not address physiological pain; requires time and cooperation [17] | Managing dental anxiety, building trust, procedural preparation [17] |
| Cold Compresses | Complements medication; empowers patient/caregiver [7] | Limited effectiveness for severe acute pain [7] | Post-surgical swelling, mild discomfort [7] |
Each method has its place in a comprehensive pain management plan, allowing professionals to tailor care to the individual needs of their young patients.
Conclusion
Managing dental pain in children effectively requires methods that align with their developmental stages. For infants, non-pharmacological techniques like sucrose solutions and swaddling can offer comfort. Meanwhile, involving adolescents in treatment decisions fosters trust and reduces anxiety, making the experience less daunting for them.
Research highlights the importance of addressing postoperative pain in young patients:
"Management of postoperative pain in children plays an important role in ensuring a smooth recovery and prompt discharge, as well as a positive dental experience." – Emily Xin Yi Ting et al., Australian Research Centre for Population Oral Health [2]
Postoperative pain is common, with around 75% of children experiencing discomfort after primary tooth extractions under general anaesthesia. Using age-appropriate tools, such as the FLACC scale for infants or numerical rating scales for older children, ensures accurate pain assessment and weight-based medication dosing [1][2].
At Complete Smiles Bella Vista, these principles are at the heart of their care. By combining evidence-based pharmacological methods with behavioural approaches, they aim to manage immediate discomfort while preventing future dental anxiety. This dual focus not only eases pain but also sets the foundation for positive dental experiences that last a lifetime.
FAQs
How do I know if my child is in dental pain if they can’t explain it?
If your child struggles to explain their pain, keep an eye out for signs like crying, irritability, difficulty eating or drinking, swelling, or sensitivity to hot or cold. These behaviours could point to dental discomfort. If you spot these symptoms, it’s a good idea to consult a dentist to identify the problem and get the right care.
Is it safe to alternate ibuprofen and paracetamol for dental pain?
Alternating ibuprofen and paracetamol can help manage dental pain in children effectively when done correctly. It’s crucial to stick to the recommended dosages and timing for each medication. If you’re ever uncertain, consult a healthcare professional for guidance. Following these steps ensures these medications are used safely to provide relief.
When would a dentist use sedation or general anaesthetic for a child?
Children who are anxious, uncooperative, or have specific dental needs may require sedation or general anaesthetic during dental procedures. Dentists often turn to these options for cases involving a strong gag reflex, special health conditions, or when local anaesthesia isn’t enough. This approach ensures treatments are carried out safely and effectively in a controlled setting.
Related Blog Posts
- 5 Pain Relief Tips for Kids’ Dental Emergencies
- Studies on Pain Management in Dental Extractions
- Pain Monitoring in Dental Surgery: Methods
- Comparing Pain Relief Methods for Kids: What Works Best?
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





