







Topical Analgesics for Neuropathic Orofacial Pain

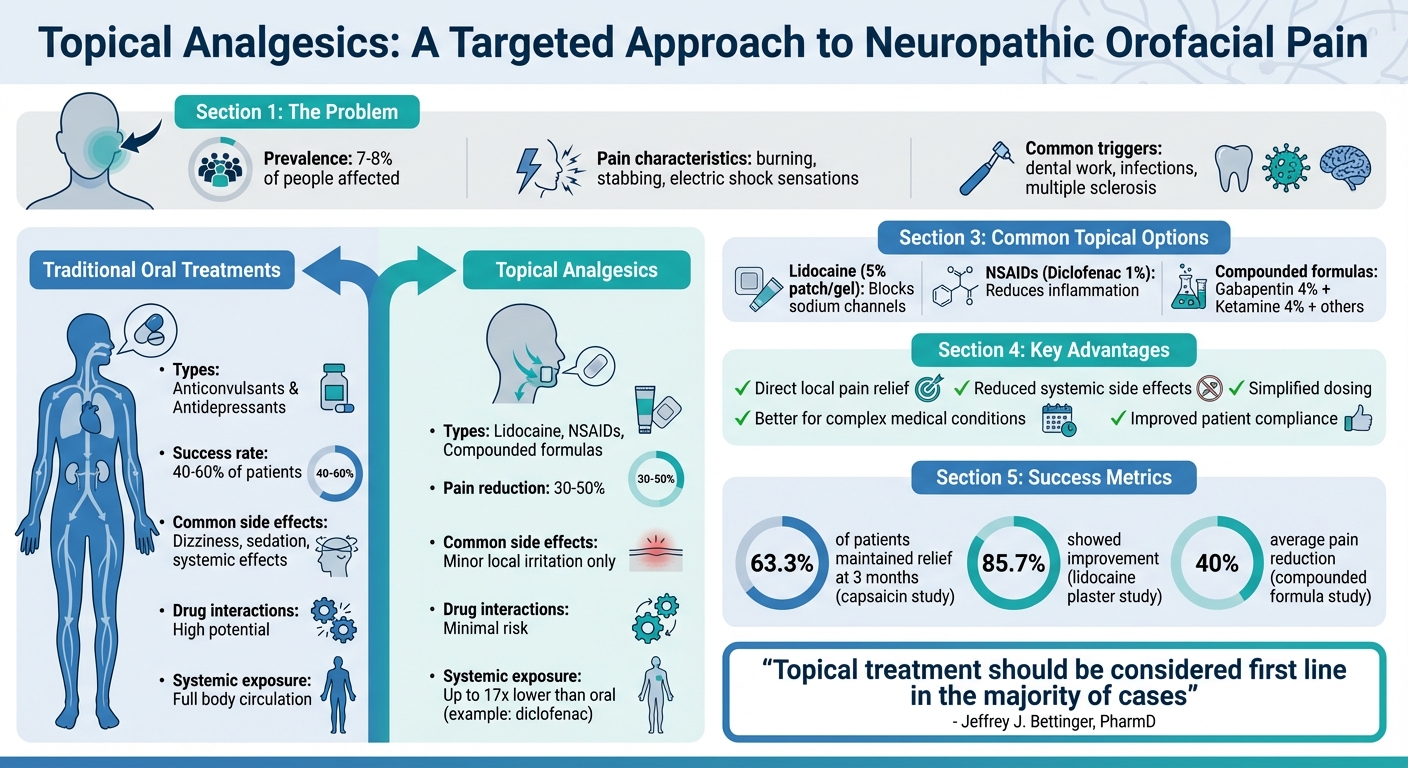
Neuropathic orofacial pain, often caused by nerve damage, affects about 7–8% of people and can feel like burning, stabbing, or electric shocks. It’s commonly triggered by dental work, infections, or conditions like multiple sclerosis. Traditional treatments, like anticonvulsants and antidepressants, help only 40–60% of patients and often cause side effects like dizziness or sedation.
Topical analgesics are a promising alternative. These treatments target pain directly at the site, avoiding many systemic side effects. Common options include lidocaine, NSAIDs, and compounded mixtures like gabapentin and ketamine. Studies show they can reduce pain by 30–50%, with minimal local irritation as the most frequent side effect. Custom stents can improve effectiveness for intra-oral applications. However, more research is needed to confirm long-term safety and effectiveness.
Key points:
- Topical analgesics work locally, reducing systemic side effects.
- Options include lidocaine, NSAIDs, and compounded formulas.
- They are particularly useful for conditions like trigeminal neuralgia and post-traumatic neuropathy.
- Clinical trials show promising results, but more long-term data is needed.
This treatment approach offers targeted relief, especially for patients who struggle with traditional medications.
Topical vs Oral Analgesics for Neuropathic Orofacial Pain: Efficacy and Side Effects Comparison
What Are Topical Analgesics
Topical analgesics are medications applied to the skin or oral mucosa, delivering concentrated relief directly to the pain site while limiting absorption into the bloodstream [3][4]. Unlike oral medications that circulate throughout the body, these treatments work locally, making them particularly useful for neuropathic orofacial pain.
The oral mucosa’s high permeability allows for quick drug absorption. However, saliva can reduce the medication’s contact time. To address this, silicone neurosensory stents are sometimes used to keep the drug in place against the affected tissue [3].
How Topical Analgesics Work
These medications are effective for managing neuropathic orofacial pain thanks to their unique mechanisms of action.
When applied, topical analgesics penetrate the skin or mucosal barrier to interact with peripheral sensory nerves. They interrupt pain pathways in several ways:
- Blocking sodium channels (e.g., lidocaine targeting Nav1.8)
- Desensitising TRPV1 receptors (e.g., capsaicin)
- Inhibiting neurotransmitter release (e.g., clonidine)
- Blocking NMDA receptors (e.g., ketamine) [4]
Since they bypass the gastrointestinal tract and liver, topical analgesics avoid first-pass metabolism, achieving higher local drug availability. For example, the systemic exposure from topical diclofenac sodium gel is up to 17 times lower than that of a 50-mg oral tablet [3].
Advantages of Topical Analgesics
These medications offer not just effective pain relief but also several practical benefits.
Their localised application reduces systemic side effects and simplifies dosing, which can improve patient adherence [4]. Unlike oral medications, they don’t typically require dose adjustments to reach therapeutic levels and carry minimal risks of drug-drug interactions. Side effects are usually limited to minor issues like local irritation or rash.
"Topical medications, in particular, may offer several advantages, including: reduced systemic side effects; lessened potential for drug-drug interactions; the ability to provide direct, local analgesia; and improved patient compliance."
– Seena Patel, DMD, MPH [4]
For patients dealing with complex medical conditions or taking multiple medications, topical analgesics provide a practical alternative to oral treatments [3].
sbb-itb-2be92ed
Common Topical Analgesics for Neuropathic Orofacial Pain
When it comes to managing neuropathic orofacial pain, there are several topical treatments available. These range from straightforward single-agent options to more complex compounded mixtures designed to tackle various aspects of pain.
Lidocaine Formulations
Lidocaine is a widely used topical analgesic, available in forms such as a 5% patch, gel, or a 2% compounded mixture. It works by blocking sodium channels in nerve membranes, which helps calm overactive nerves and reduces the abnormal discharges that cause sensations like burning or stabbing pain [2][3]. This makes it particularly effective for conditions involving localised peripheral sensitisation, including postherpetic neuralgia, trigeminal neuralgia, and neuralgia following surgery or trauma [2][7].
Patients with allodynia often find relief with lidocaine. One advantage of the 5% lidocaine patch is that it alleviates pain without causing complete numbness, which can make it more appealing compared to some anaesthetic creams [4].
Topical NSAIDs
Topical NSAIDs work by reducing inflammation locally. They achieve this by inhibiting cyclooxygenase enzymes, which are involved in the production of inflammatory mediators like prostaglandins. Common options include diclofenac (1%) and ketoprofen (4%) [4]. These are particularly useful when pain is driven by tissue damage, which can create a "sensitising soup" of inflammatory mediators.
Studies have shown that topical diclofenac is as effective as its oral counterpart for treating temporomandibular joint symptoms but with significantly fewer systemic side effects [4]. This makes it a safer option for many patients.
When single-agent treatments fall short, compounded formulations offer a more tailored approach by targeting multiple pain pathways at once.
Compounded Analgesics
For patients with complex or stubborn pain, compounded formulations combine several active ingredients to address different pain mechanisms simultaneously. Commonly included agents are gabapentin (4%), pregabalin (5–10%), ketamine (4%), and amitriptyline (2%). Gabapentin and pregabalin work by acting on the alpha-2 delta subunit of voltage-gated calcium channels, reducing the release of excitatory neurotransmitters like glutamate [2][3]. Ketamine, an NMDA receptor antagonist, helps decrease central sensitisation, while amitriptyline serves as both a sodium channel blocker and a cholinergic receptor antagonist.
These combinations are particularly effective for conditions such as post-traumatic trigeminal neuropathic pain, sympathetically maintained pain, and persistent idiopathic facial pain [2][3].
In one notable case from December 2021, researchers at the Rutgers School of Dental Medicine treated a 34-year-old man suffering from severe burning pain (10/10) following a maxillary third molar extraction. A compounded formulation containing lidocaine, ketoprofen, gabapentin, pregabalin, and ketamine was applied using a neurosensory stent. Remarkably, the patient experienced complete pain relief within five minutes, and the relief lasted for six months [2].
For intra-oral applications, a custom silicone stent can be used to ensure prolonged contact between the medication and the affected tissue [2][3].
Clinical Research Findings
Recent studies highlight the effectiveness and safety of topical analgesics in managing neuropathic orofacial pain – a condition where standard treatments often fall short.
Pain Relief Outcomes
Research confirms that topical analgesics can offer meaningful relief for neuropathic orofacial pain, though the strength of evidence varies by product. High-dose capsaicin (8%) and lidocaine topical systems (5% or 1.8%) have the most robust research backing and are FDA-approved for specific neuropathic conditions like postherpetic neuralgia [5].
"Topical treatment should be considered first line in the majority of cases (especially for those products that have FDA approvals)" – Jeffrey J. Bettinger, PharmD, Pain Management Clinical Pharmacist [5]
A reduction of 50% in pain is considered a successful intervention, while a 30% reduction is deemed clinically meaningful [3]. A retrospective study involving 39 patients with various orofacial neuropathic conditions found that a compounded topical formula (containing carbamazepine, lidocaine, ketoprofen, ketamine, and gabapentin) achieved a 40% pain reduction [4]. In another trial, 0.025% capsaicin was evaluated for painful post-traumatic trigeminal neuropathy, with 19 out of 30 patients (63.3%) maintaining pain relief after three months [4]. Similarly, a small case series of 14 patients with extraoral trigeminal neuropathic pain treated with 5% lidocaine plasters showed improvement in 12 patients (85.7%) [4]. These results are particularly significant given that 40% to 60% of patients with neuropathic pain report inadequate relief from conventional oral medications [5]. These promising outcomes are further supported by the generally benign safety profile of these treatments.
Safety and Side Effects
The safety profile of topical analgesics is generally well-tolerated, with most adverse effects limited to the application site. Minimal systemic absorption greatly reduces the risk of systemic side effects [5]. In a study of 508 participants across 12 trials, no evidence suggested that topical lidocaine increased adverse events compared to a placebo [7].
The most common side effects are localised reactions like redness, rash, or burning at the application site [4][5]. Capsaicin, particularly at an 8% concentration, often causes intense local burning and stinging, which can lead to low adherence to treatment [4]. However, systemic exposure from topical agents remains minimal; for instance, systemic absorption of diclofenac sodium gel (1%) is up to 17 times lower than that of a 50-mg oral tablet [3]. Rarely, certain agents like clonidine may cause systemic effects such as sedation or low blood pressure if absorbed in significant amounts, necessitating closer monitoring [4].
Guidelines for Using Topical Analgesics
Applying topical analgesics correctly and following dosing schedules are key to managing neuropathic orofacial pain effectively. The oral environment poses unique challenges, such as reduced contact time, which means specific techniques are needed to maintain the medication’s effectiveness [3].
Application and Dosing Instructions
For intra-oral applications, topical anaesthetics mixed with a methylcellulose paste (like orobase) need to be applied 4–6 times a day to maintain effective drug levels [4]. To prevent the medication from being washed away by saliva, custom-made silicone stents can be used to hold it in place against the affected tissue [2].
For extra-oral applications, the instructions vary depending on the medication:
- Lidocaine 5% patches: These are generally used on a 12-hour schedule – 12 hours on, followed by 12 hours off [4].
- Diclofenac gel 1%: This can be applied to areas like the temporomandibular joint or the masseter region up to four times daily, using no more than 1 gram per application [4].
- Capsaicin (0.025%–0.075%): Applied 3–4 times daily, patients should be informed about the initial burning sensation and reminded to wash their hands thoroughly after each use [8].
For Burning Mouth Syndrome, a swish-and-spit method with dissolved clonazepam (0.5 mg) three times daily is recommended. This ensures the medication coats the entire oral cavity before being expelled [4]. Additionally, gels containing Poloxamer 407 are designed to thicken at body temperature (37°C) for better adhesion. These should be stored as advised by the pharmacy to maintain their properties [3].
These carefully designed dosing strategies are critical for tailoring treatments to meet individual patient needs.
Custom Compounding Options
Compounding pharmacies can create specialised formulations to address specific patient requirements. For example, a gel combining ketamine 4%, gabapentin 4%, and lidocaine 1% targets multiple pain receptors simultaneously, which may benefit patients who haven’t responded well to single-agent treatments [4][2]. To enhance absorption, these formulations often use advanced bases like Lipoderm or Pluronic Lecithin Organogel (PLO) [1][2].
To improve adherence to intra-oral treatments, pharmacies may include sweeteners (like saccharin or xylitol) and flavouring oils (such as orange, peppermint, or tangerine) [3][2]. However, as Jeffrey J. Bettinger, PharmD, cautions:
"Because there is very little data on most compounded topicals (not just efficacy data, but pharmacokinetic data), there can be inconsistencies batch to batch, depending on the medication being compounded" [5].
Patients should also monitor the texture of their compounded medications. If the formulation becomes gritty or uneven, it may indicate that the active ingredients are no longer fully dissolved, which could reduce its effectiveness [3].
Gaps in Current Research
Research on topical analgesics for neuropathic orofacial pain is still quite limited. A 2024 review found only 14 manuscripts focused on topical treatments for intra-oral post-traumatic trigeminal neuropathic pain [3]. Much of the available data comes from expert opinions, case reports, and small case series, rather than robust, large-scale, double-blind randomised controlled trials [3][4].
One major issue is the absence of long-term follow-up data. Most trials report results for up to four weeks, leaving questions about long-term safety and efficacy unanswered. For example, a study on atypical odontalgia showed that 19 out of 30 patients experienced relief after four weeks of capsaicin treatment, yet the original sample size was 50 [4]. Researchers have pointed out that small sample sizes, inconsistent methodologies, and a reliance on subjective opinions highlight the urgent need for more rigorous and standardised research [3].
The oral environment itself poses unique challenges for topical treatments. Most existing data on topical analgesics are derived from studies on skin applications, but the oral mucosa is up to 10 times more permeable and subject to constant salivary washout [3]. This makes it difficult to translate findings directly to intra-oral use. Moreover, there is often a disconnect between clinical symptoms and the biological mechanisms causing the pain. Many trials adopt a "one-size-fits-all" approach, without distinguishing whether the pain stems from peripheral or central sensitisation [9]. To address this, future research should incorporate quantitative sensory testing and use standardised delivery systems, such as neurosensory stents, to identify which patients are most likely to benefit from specific treatments [3][6].
Another area needing exploration is the variability in patient responses. Early evidence suggests that women may respond better to certain combinations – like lidocaine, pregabalin, and ibuprofen – but larger studies are required to confirm these trends [10]. As the European Pain Federation observes:
"Not all individuals respond to topical analgesics, and there is interest in determining factors (patient factors, sensory characteristics) which might predict responsiveness to topical analgesics" [6].
These gaps underscore the importance of developing personalised treatment strategies that consider individual patient characteristics and the unique challenges posed by the oral environment.
Conclusion
Topical analgesics offer a targeted way to manage neuropathic orofacial pain conditions – like trigeminal neuralgia, post-traumatic neuropathy, and burning mouth syndrome – by delivering medication directly to the affected area. This approach avoids first-pass metabolism and minimises systemic side effects, making it especially helpful for older adults, those with multiple health conditions, or individuals needing to stay alert for work.
There’s growing support for using agents like lidocaine, capsaicin, and compounded formulations in clinical settings.
"Topical treatment should be considered first line in the majority of cases (especially for those products that have FDA approvals)"
– Jeffrey J. Bettinger, PharmD, Pain Management Clinical Pharmacist [5]
Still, challenges like salivary washout and differences in mucosal permeability highlight the need for advanced delivery systems, such as neurosensory stents. While early findings are promising, much of the current evidence comes from smaller studies and expert opinions, leaving gaps in large-scale, long-term data.
Future research should aim to standardise application methods, explore new therapies like cannabinoids, and create more personalised treatment options. A patient-focused approach remains key – this means considering individual lifestyles, conducting thorough assessments, and tailoring treatments to improve adherence. Combining current knowledge with future advancements will ultimately lead to better outcomes and improved quality of life for patients.
FAQs
Are topical analgesics safe to use inside the mouth?
Topical analgesics, when used properly, are typically safe for intra-oral applications. They offer focused pain relief while keeping the risk of systemic side effects low. That said, some formulations lack extensive research, underlining the importance of further studies to validate their safety and effectiveness. It’s always best to use these treatments under professional advice.
How do I know if my facial pain is neuropathic or something else?
Neuropathic orofacial pain can feel like burning, stabbing, or even electric shock-like jolts. It may also come with unusual symptoms such as allodynia (pain triggered by something that wouldn’t normally hurt, like a light touch) or hyperalgesia (when normal pain feels much more intense than it should).
Diagnosing this condition isn’t straightforward – it calls for a thorough clinical evaluation. This includes reviewing your medical history, especially if there’s been any trauma or nerve damage in the area. If you’re experiencing these kinds of symptoms or noticing changes in sensation, it’s crucial to reach out to a healthcare professional who specialises in orofacial pain. They can provide the right diagnosis and help you manage the condition effectively.
What should I ask my dentist or doctor before trying a compounded topical cream or gel?
Before trying a compounded topical cream or gel for neuropathic orofacial pain, it’s important to have a conversation with your dentist or doctor. Here are a few key points to cover:
- Ingredients and risks: Find out exactly what’s in the medication and whether there’s any chance of an allergic reaction or other risks.
- Safety and effectiveness: Ask if the cream or gel has been properly evaluated to ensure it’s both safe and works as intended.
- Side effects and interactions: Discuss potential side effects, how it might interact with other medications you’re taking, and whether it’s a good fit for your overall health.
Make sure to also review how to use it correctly, the right dosage, and steps to take if you experience any adverse reactions.
Related Blog Posts
- Neurostimulation: Future of Dental Pain Relief
- How Combination Analgesics Manage Orofacial Pain
- Neuropathic Orofacial Pain: Adjuvant Analgesic Options
- Emerging Therapies in Orofacial Pain Management
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





