







Top Factors Affecting Apex Locator Accuracy
Electronic Apex Locators (EALs) are essential for determining the working length in root canal treatments. Their accuracy is influenced by multiple factors, including operator technique, anatomical variations, and procedural considerations. Here’s a quick breakdown of what matters most:
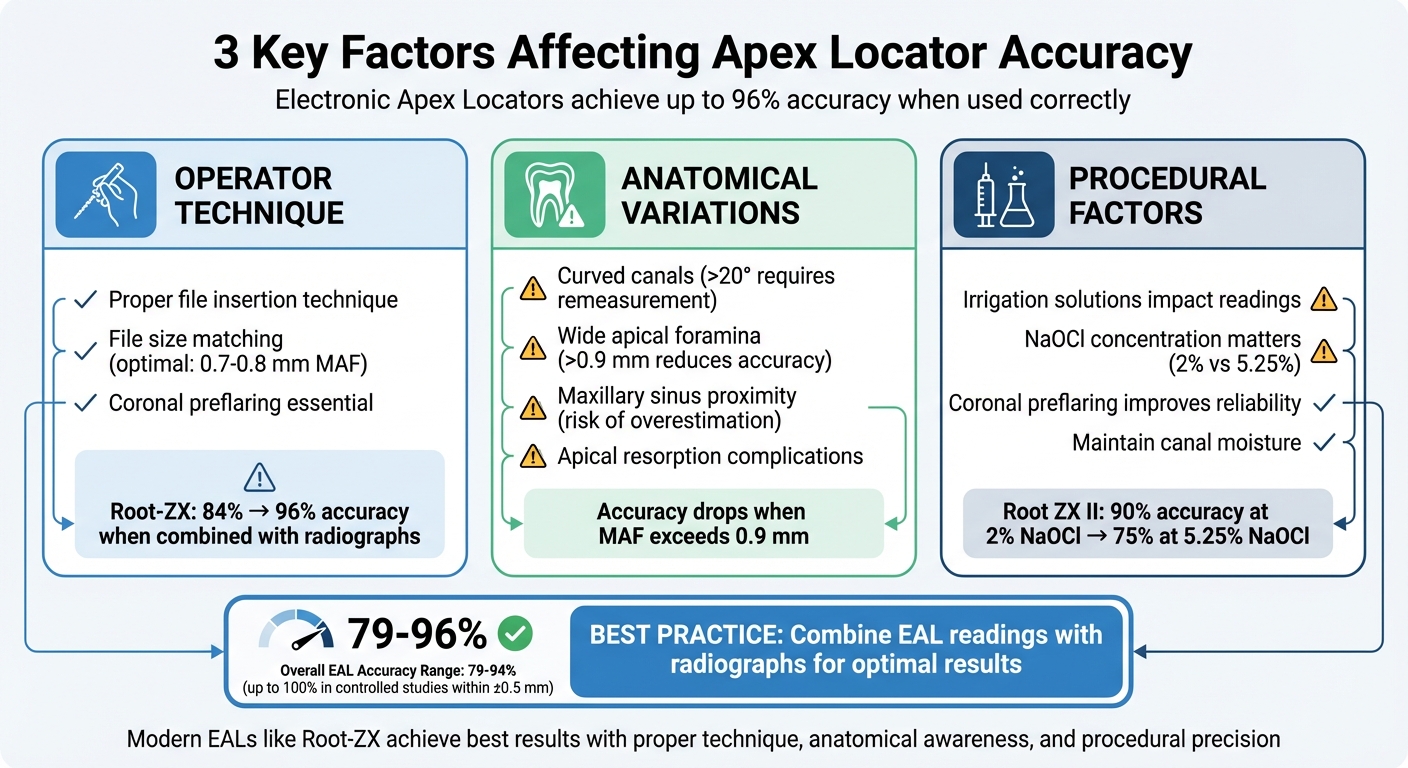
- Operator Technique: Proper file insertion, coronal preflaring, and file size matching are key to precise readings. Over-insertion or poor file fit can lead to errors.
- Anatomical Variations: Curved canals, wide apical foramina, and proximity to the maxillary sinus can affect accuracy. Adjustments and radiographic confirmation help mitigate these challenges.
- Procedural Factors: Irrigation solutions like sodium hypochlorite and chlorhexidine can impact readings, especially at higher concentrations. Coronal preflaring and maintaining canal moisture improve reliability.
Modern EALs, such as the Root-ZX, achieve up to 96% accuracy when combined with radiographs. However, achieving consistent results requires understanding these factors and using the right techniques.
Key Takeaway: Combining EAL readings with radiographs and refining operator skills ensures better outcomes in root canal treatments.
Three Key Factors Affecting Apex Locator Accuracy in Root Canal Treatment
Working Lengths and Troubleshooting Apex Locators – PDP216
sbb-itb-2be92ed
1. Operator Technique
How a clinician handles an apex locator plays a key role in the accuracy of its readings. Even the most advanced devices can give unreliable results if not used correctly.
Impact on Accuracy
The method of file insertion is crucial. Advancing the file directly to the "apex" reading ensures accuracy. Over-insertion, however, can alter the major apical foramen (MAF) and disrupt the electrical circuit, leading to incorrect readings[5].
File selection and fit also matter. The file should fit snugly in the apical area. For optimal results, the file size should match the MAF, ideally between 0.7–0.8 mm. When the MAF exceeds 0.9 mm, accuracy drops regardless of the file used. In cases of wide canals or immature apices, using an undersized file can result in unstable or incorrect readings due to inconsistent contact with the canal walls[5].
Coronal preflaring is another important step. It reduces binding in the upper canal, improving tactile feedback and enhancing the precision of the device’s readings[5][7].
Supporting Evidence
Studies highlight the importance of combining apex locator readings with radiographic confirmation. For example, the Root-ZX device identifies the apical constriction with 84% accuracy on its own, but this increases to 96% when radiographs are used alongside it[1]. Overall, electronic apex locators show accuracy rates ranging from 79% to 94%[4], with some controlled studies reporting up to 100% accuracy within ±0.5 mm[6].
"The devices are most accurate at determining the apical limit when the attached endodontic file contacts the periodontal ligament space and the visual analogue displays ‘Apex’ or ‘0’."
- Ali et al.[2]
Recent findings suggest that advancing the file to the "0.0" (apex) reading and then subtracting 0.5 mm clinically provides a better estimation of the true working length compared to relying solely on the device’s "0.5" mark[3].
Mitigation Strategies
To optimise accuracy, prepare the chamber by drying the pulp and maintaining canal moisture with an irrigant[5][7]. Be cautious with conductive solutions like sodium hypochlorite; flooding the chamber can cause short-circuiting, especially if the fluid contacts metallic restorations.
Prevent false "apex" signals by avoiding file contact with metallic restorations. If interference is likely, use insulation techniques to minimise errors[7].
For curved canals (over 20°), re-measure the working length throughout the cleaning and shaping process. As the canal straightens, the effective length may change. Always verify apex locator readings with radiographs and keep in mind the average tooth lengths for additional confirmation[5][8].
2. Anatomical Factors
The natural variations in tooth anatomy can influence the performance of apex locators, often requiring adjustments to techniques to minimise measurement errors. Let’s delve into how specific anatomical features can impact these measurements.
Impact on Accuracy
Root canal curvature has a significant effect on measurement precision. When the curvature is excessive (over 20°), the increased contact between the file and canal walls can reduce accuracy. However, moderate curvatures (ranging from 9° to 58°) generally maintain reliable measurements[5].
Foramen diameter is another critical factor. Measurement reliability decreases as the major apical foramen (MAF) widens beyond 0.6 mm and drops sharply when it exceeds 0.9 mm. Additionally, lateral foramina often lead to overextended "Apex" readings, while "0.5" readings tend to remain dependable[5].
Proximity to the maxillary sinus presents unique challenges. Roots located near or extending into the maxillary sinus – particularly palatal roots – are prone to length overestimations due to changes in impedance. This increases the risk of over-instrumentation in these areas[5].
"The proximity of the maxillary sinus to a root end can also affect the length estimation accuracy." – Shayan Golkar et al.[5]
Apical resorption can further complicate measurements by widening the MAF and altering impedance readings. While some studies report significant impacts in cases of immature or blunderbuss apices, others have found minimal effects[5][7].
Supporting Evidence
In more complex anatomies, such as C-shaped canals, electronic apex locators (EALs) tend to overestimate lengths by about 7.3%, compared to 20% when using radiography[1]. For instance, the Root ZX device demonstrated 100% accuracy within ±0.5 mm in maxillary premolars, outperforming digital radiography, which achieved 84.48% accuracy[6]. Additionally, the distance between the apical constriction and the foramen varies with age, averaging 0.5 mm in younger patients and up to 0.8 mm in older individuals, requiring clinicians to make appropriate adjustments[1].
Mitigation Strategies
To address these challenges:
- For canals with an MAF larger than 0.7 mm, use a file that matches the foramen diameter.
- When a lateral foramen is suspected, rely on the "0.5" reading to avoid over-instrumentation[5].
- In curved canals with angles exceeding 20°, remeasure after shaping.
- For roots near the maxillary sinus, confirm EAL readings with radiographs to ensure accuracy.
- In older patients, extend the working length slightly to account for the increased distance between the apical constriction and the foramen[1][5].
3. Procedural and Material Factors
When it comes to apex locator precision, the materials used and procedural methods applied are just as crucial as operator techniques and anatomical differences.
Impact on Accuracy
Irrigation solutions play a significant role in influencing readings due to their conductivity. For instance, sodium hypochlorite (NaOCl), with its high electroconductivity, reduces electrical impedance, often leading to shorter length measurements. Increasing NaOCl concentration from 2% to 5.25% can lower the accuracy of devices like Root ZX II and Apex ID from 90% to 75% within a ±0.5 mm margin[9]. On the other hand, chlorhexidine (CHX), which has poor electrical conductivity, tends to cause overestimations by producing longer measurements[10]. Heated 5% NaOCl is particularly problematic, as it increases free chlorine and conductivity, resulting in the lowest accuracy among tested solutions[10].
Dentinal debris can interfere with readings, reducing accuracy, while blood in the root canal has been shown to have no significant effect on modern multi-frequency devices[5]. Coronal preflaring, which involves removing cervical constraints, significantly improves the accuracy of working length determination. This has been confirmed by 11 separate studies[5]. Additionally, file selection becomes critical in wider canals; accuracy decreases when the major apical foramen exceeds 0.7 mm unless the file size closely matches the foramen diameter[5].
"The presence of different irrigating media in the RCS does not impact significantly on the performance of third/fourth generation apex locators." – Ali et al.[2]
These factors are supported by quantifiable data that highlight their influence on apex locator performance.
Supporting Evidence
In tests using 2% NaOCl, the Root ZX II demonstrated 90% accuracy within ±0.5 mm. However, this dropped to 75% when the concentration increased to 5.25%[9]. Interestingly, the Dual Pex device achieved 100% accuracy in 5.25% NaOCl under specific operators, suggesting that multi-frequency technology can sometimes benefit from higher electrolyte concentrations[9]. Overall, electronic apex locators achieve an accuracy rate of 83% to 92% within a 0.5 mm range across various canal conditions[11]. Notably, the type of file alloy – whether stainless steel or nickel-titanium – does not appear to significantly affect accuracy[5].
Mitigation Strategies
To address these challenges, consider the following protocols:
- After using sodium hypochlorite or chlorhexidine, apply 17% EDTA to reduce the negative effects of high electroconductivity[10].
- While modern apex locators can function in wet canals, it’s a good idea to dry the pulp chamber with cotton pellets while keeping the root canal moist for consistent readings[9][12].
- Perform coronal preflaring before taking electronic measurements to enhance device reliability[5][12].
- Stop at the "0.0" or "Apex" reading to avoid over-instrumentation[5].
These strategies can help ensure more reliable and accurate results when using apex locators.
Advantages and Disadvantages
When it comes to how apex locators measure performance, clinicians need to strike a balance between factors they can control and those that are inherent. These include operator technique, anatomical variations, and procedural elements.
Operator technique plays a key role in improving accuracy. For instance, proper coronal preflaring significantly enhances precision[5]. Ensuring the file diameter closely matches the major apical foramen is especially effective in canals with diameters between 0.7 mm and 0.8 mm[5]. However, using an "over-and-back" approach – where the file is pushed slightly beyond the apex and then withdrawn – can enlarge the foramen, reducing the reliability of measurements[5].
Anatomical factors present challenges that are harder to manage. While the Root ZX device has demonstrated 100% accuracy within ±0.5 mm under controlled conditions[6], larger apical diameters (ranging from 0.6 mm to 0.9 mm or more) can compromise precision[5]. Interestingly, the position of the apical foramen – whether central or lateral – has minimal impact on the accuracy of electronic apex locators, which outperform radiographic methods in reliability[6].
Material and procedural factors have little influence on modern apex locators. Third and fourth-generation devices are designed to resist interference from irrigating solutions, such as sodium hypochlorite, maintaining their accuracy regardless of the solution used[5]. The main limitation arises in canals with larger apical foramina (over 0.9 mm), where accuracy diminishes, regardless of the file size or material[5].
"The precision of electronic WL measurement depends on the device used and the type of irrigation and is not influenced by the status of the pulp tissue (vital or necrotic)." – Tsesis et al.[7]
Conclusion
Electronic apex locators (EALs) boast an impressive accuracy rate of 90% in clinical settings [4]. However, their effectiveness heavily depends on the operator’s technique. Key factors like proper coronal preflaring and the selection of the correct file size play a critical role in achieving reliable results [5][12].
Certain anatomical challenges can complicate the process. For example, when the diameter of the major apical foramen exceeds 0.6 mm to 0.9 mm, accuracy diminishes, regardless of the operator’s skill [5]. Similarly, maxillary molars with roots positioned close to the sinus present a risk of overestimation. In such cases, combining EAL readings with periapical X-rays is essential. This dual approach significantly improves precision, raising accuracy from 84% to 96% [1].
Modern materials and irrigants have also streamlined the process. Substances like sodium hypochlorite and chlorhexidine do not interfere with EAL readings [5][12]. However, for the best results, it’s important to keep the pulp chamber dry while ensuring the canal remains moist to maintain optimal conductivity [12][4].
It’s worth noting that apex locators should always be used alongside radiographs [5][1]. This combination helps mitigate the limitations of each method, particularly in cases involving complex anatomical structures.
"Although the accuracy of EALs is acceptable in most cases, the use of radiography along with EALs remains advisable to confirm the measurement in clinical scenarios." – Shayan Golkar, Department of Endodontics, School of Dentistry, Isfahan University of Medical Sciences [5]
Ultimately, a combined approach that leverages both operator expertise and confirmatory radiographs is the best way to ensure successful endodontic outcomes.
FAQs
What factors in operator technique can impact the accuracy of an apex locator?
The effectiveness of an electronic apex locator (EAL) largely hinges on the operator’s technique. For accurate readings, it’s crucial to insert the file gently and steadily until it reaches the apical constriction. Choosing the right file size and carefully interpreting the device’s signals also play a key role in ensuring precise measurements. Applying excessive pressure or prematurely withdrawing the file can disrupt the electrical circuit, leading to unreliable results.
Additional techniques that enhance accuracy include pre-flaring the canal to reduce its curvature, maintaining apical patency, and steering clear of irrigants that might alter the canal’s conductivity. Sticking to the manufacturer’s instructions for the specific EAL model is equally important, especially with newer devices designed to perform consistently under varying canal conditions. By following these practices, clinicians can minimise reliance on additional X-rays while achieving dependable and consistent outcomes.
What factors in tooth anatomy can influence the accuracy of an apex locator?
The reliability of apex locators can be affected by various anatomical factors. These include the curvature and length of the root canal, the specific type of tooth undergoing treatment, and the closeness of nearby structures like the maxillary sinus. Other influential factors include variations in the size and shape of the apical foramen, the presence of lateral or accessory canals, instances of internal root resorption, perforations, and differences in apical patency.
Recognising these factors is essential for obtaining accurate measurements during root canal procedures, which directly impacts the quality of treatment outcomes.
How do irrigation solutions impact the accuracy of an apex locator?
Irrigation solutions can affect how accurately electronic apex locators work by changing the electrical conductivity inside the root canal. For instance, sodium hypochlorite and chlorhexidine might decrease the accuracy of these devices when compared to dry conditions or the use of saline. In contrast, some solutions like QMix are reported to provide more consistent and dependable readings.
Knowing how various solutions interact with apex locators is key to getting precise measurements during root canal treatments. If you’re uncertain about the most suitable option, seeking advice from a dental professional can help ensure the best results.
Related Blog Posts
- Real-Time Feedback in Ultrasonic Endodontics
- How Apex Locators Measure Root Canal Length
- How Irrigation Solutions Affect Apex Locator Accuracy
- Clinical Benefits of Ultrasonic Root Canal Devices
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





