







Porcelain vs. Ceramic: Strength and Fracture Resistance

Porcelain and ceramics are popular materials in dentistry, offering aesthetic and durable solutions for restoring teeth. However, their strength and fracture resistance differ significantly, making material selection critical based on use and location in the mouth. Here’s a quick breakdown:
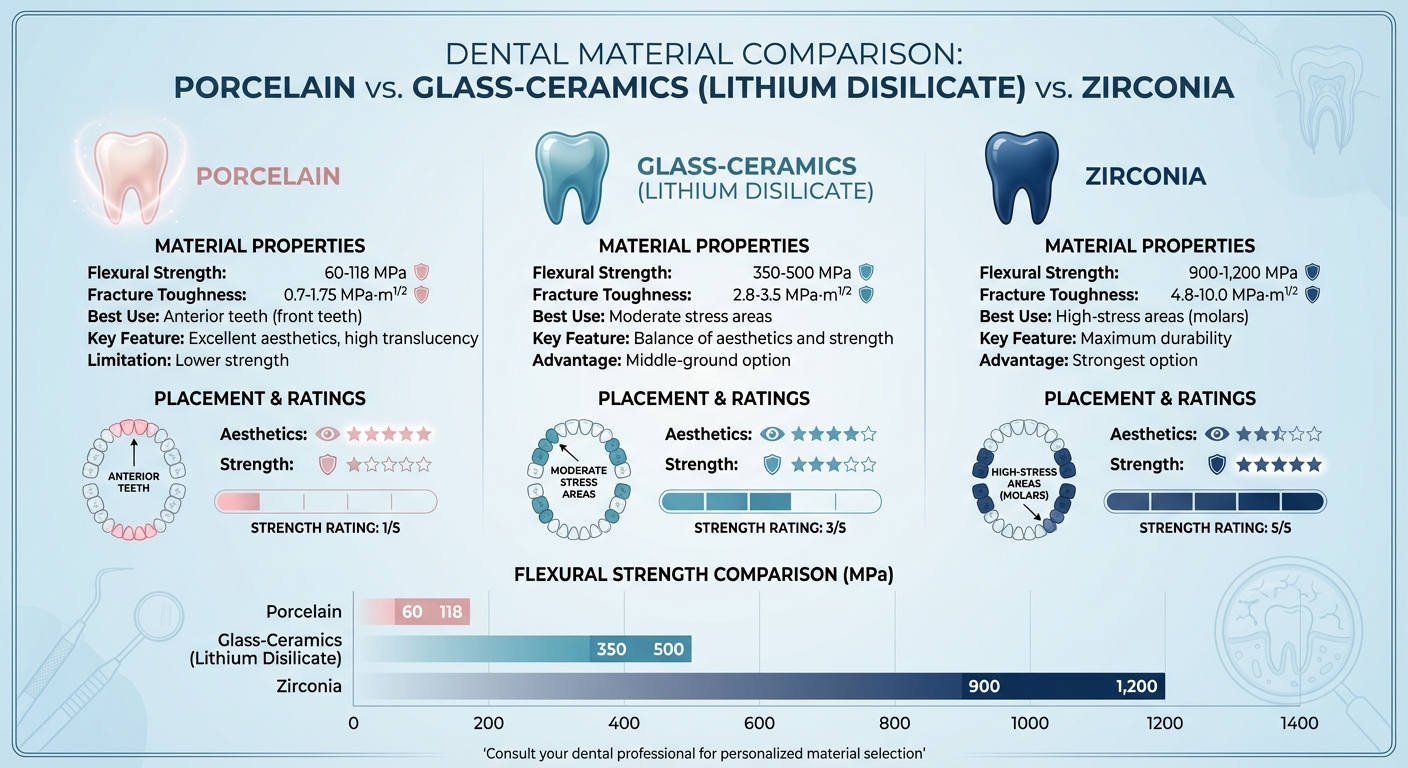
- Porcelain: Known for its translucency, it is ideal for front teeth but has lower strength and fracture resistance due to its glassy structure. Flexural strength ranges from 60–118 MPa, and fracture toughness is ~0.7–1.75 MPa·m¹/².
- Glass-Ceramics (e.g., Lithium Disilicate): A balance of aesthetics and strength, suitable for moderate stress areas. Flexural strength is 350–500 MPa, with fracture toughness of ~2.8–3.5 MPa·m¹/².
- Zirconia: The strongest option, ideal for molars and high-stress areas. Flexural strength exceeds 900–1,200 MPa, and fracture toughness ranges from 4.8–10.0 MPa·m¹/².
Key Takeaway: Porcelain excels in aesthetics but lacks strength, while zirconia offers unmatched durability for high-stress areas. Lithium disilicate is a middle-ground option for both strength and appearance.
Quick Comparison
| Material Type | Flexural Strength (MPa) | Fracture Toughness (MPa·m¹/²) | Best Use |
|---|---|---|---|
| Porcelain | 60–118 | ~0.7–1.75 | Anterior teeth |
| Glass-Ceramics | 350–500 | ~2.8–3.5 | Moderate stress |
| Zirconia | 900–1,200 | ~4.8–10.0 | High-stress areas |
For personalised advice, consult a dental professional to ensure the right material is chosen for your needs.
Dental Material Strength Comparison: Porcelain vs Ceramics vs Zirconia
Material Composition and Properties
Porcelain Composition and Characteristics
Traditional feldspathic porcelain is made up of potash and soda feldspar, quartz, and kaolin. Together, these ingredients create a three-dimensional silica network with a predominantly glass-based, amorphous structure. This structure is what gives porcelain its well-known translucency, making it a popular choice for veneers and crown veneers.
But this glassy nature has its downsides. As M.M. Barrelro points out:
Dental feldspathic porcelain is predominantly a glass material with an amorphous (non‑crystalline) structure [3].
This amorphous structure makes it highly sensitive to surface flaws and defects, which can lead to rapid crack propagation. Typically, traditional feldspathic porcelain has flexural strengths ranging from 60 to 118 MPa and fracture toughness values of about 0.7–1.0 MPa·m^0.5 [5] [8].
Fortunately, modern ceramics have been developed to address these vulnerabilities.
Ceramic Composition and Characteristics
Modern dental ceramics encompass a wide variety of materials with differing ratios of glass to crystalline content. One example is glass-ceramics, such as lithium disilicate, which is composed of roughly 70% crystalline lithium disilicate and 30% amorphous silica [7]. Its structure features interlocking, needle-like crystals embedded in a glass matrix. As Arvind Shenoy explains:
The needle‑like crystals cause cracks to deflect, branch or blunt; thus, the propagation of cracks through this material is arrested by the lithium disilicate crystals, providing a substantial increase in the flexural strength [5].
This unique microstructure gives lithium disilicate glass-ceramics flexural strengths of 360–500 MPa and fracture toughness values between 2.8 and 3.5 MPa·m^0.5 [7].
Polycrystalline ceramics, on the other hand, offer even greater strength. Zirconia, a type of polycrystalline ceramic, stands out as the strongest option in this category. Unlike glass-ceramics, zirconia contains no glass phase and is made entirely of sintered zirconium oxide crystals. These crystals are stabilised with dopants like yttria (3–8 mass%) to maintain their tetragonal phase at room temperature [5]. During firing, zirconia undergoes approximately 30% volumetric shrinkage (or about 10% linear shrinkage) to achieve full density [5]. This results in a dense, air-free structure that allows zirconia to achieve flexural strengths exceeding 900–1,200 MPa and fracture toughness values of 8.0–10.0 MPa·m^0.5 [1] [7].
What sets zirconia apart is its transformation toughening mechanism. When stress is applied at a crack tip, the tetragonal grains transform into a monoclinic phase, causing a 4.4% volume increase. This expansion essentially "squeezes" the crack closed, enhancing the material’s resistance to fracture [5].
Strength and Fracture Resistance Comparison
Flexural Strength
Dental materials show a broad range of flexural strengths. Traditional feldspathic porcelain falls between 60.7 MPa and 82.7 MPa [1]. Leucite-reinforced glass-ceramics, like IPS Empress, are stronger, with values ranging from 106 MPa to 133.5 MPa [9]. Lithium disilicate ceramics take it a step further, boasting flexural strengths of 350 MPa to 450 MPa [5]. At the top of the spectrum, zirconia-based ceramics dominate with strengths between 840 MPa and 1,140.89 MPa [9].
These differences stem from each material’s structure. Porcelain’s glassy composition limits its strain tolerance to just 0.1%–0.2% [5]. On the other hand, zirconia benefits from transformation toughening, which significantly boosts its strength. To get a fuller picture, let’s look at fracture resistance next.
Fracture Toughness
Fracture toughness reveals how well a material resists crack growth. Dental porcelains generally have low fracture toughness, around 1.33 to 1.75 MPa·m¹/² [3][8]. Leucite glass-ceramics are similar, with values of 1.2 to 1.33 MPa·m¹/² [9]. Lithium disilicate ceramics improve on this, offering toughness between 2.9 and 3.0 MPa·m¹/² [5]. However, zirconia-based ceramics lead the pack, with fracture toughness ranging from 4.8 to 7.4 MPa·m¹/² [9].
As noted by Guazzato et al. in the Dental Materials Journal:
"The zirconia-based dental ceramics are stronger and tougher materials than the conventional glass-ceramics. Better properties can have positive influence on the clinical performance of all-ceramic restorations." [9]
Zirconia owes this toughness to its stress-induced phase transformation, which creates compressive forces that counteract crack propagation. This makes it far more resistant to surface flaws compared to porcelain.
Comparison Table
Here’s a summary of the key performance metrics for these materials:
| Material Type | Specific Example | Flexural Strength (MPa) | Fracture Toughness (MPa·m¹/²) |
|---|---|---|---|
| Feldspathic Porcelain | Vita VMK 68 / Alpha | 60.7 – 82.7 [1] | ~1.75 [3] |
| Leucite Glass-Ceramic | IPS Empress | 106 – 133.5 [9] | 1.2 – 1.33 [9] |
| Lithium Disilicate | IPS e.max (Empress 2) | 350 – 450 [5] | 2.9 – 3.0 [5] |
| Glass-Infiltrated Alumina | In-Ceram Alumina | 429.3 – 594 [9] | 3.6 – 4.4 [9] |
| Zirconia (Y-TZP) | Cercon / DC-Zirkon | 840 – 1,140.89 [9] | 4.8 – 7.4 [9] |
Predictability and Reliability
Industrial ceramics, such as those used in CAD/CAM systems, offer greater structural reliability compared to lab-processed porcelains. For instance, materials like Cerec Mark II and Zirconia-TZP often achieve Weibull modulus values above 18, indicating highly consistent performance. In contrast, laboratory-fabricated porcelains typically range between 5 and 15 [1]. This predictability makes industrially manufactured ceramics a preferred choice for clinical applications.
Material Selection Factors in Dental Applications
Aesthetic Requirements vs. Functional Demands
When selecting materials for dental restorations, it’s all about finding the right balance between appearance and function. For example, the forces at play in different parts of the mouth vary significantly. Anterior restorations experience lower chewing forces, typically between 110–150 N, with peaks of around 200 N. In contrast, posterior teeth, especially molars, endure forces of up to 350 N, and this can increase further in patients with bruxism [7].
For anterior teeth, glass-based lithium disilicate is a popular choice. Its excellent translucency makes it ideal for visible areas, and it provides enough strength to handle the lower forces in these regions [7]. On the other hand, polycrystalline ceramics like zirconia, with a flexural strength of about 1,039 MPa [7], are better suited for molars and premolars where durability is critical. As emphasised by Loo Chien Win, Peter Sands, Stephen J Bonsor, and FJ Trevor Burke in the Dental Materials Journal [7]:
With different load forces on the anterior and posterior regions, it is obvious that the same ceramic material cannot be considered for use in every patient.
The next step in material selection involves evaluating how these materials interact with natural teeth.
Biocompatibility and Wear on Opposing Teeth
Porcelain and ceramic materials are not only biocompatible but also chemically stable, avoiding the complications often associated with metal restorations [5][6]. However, their interaction with opposing teeth varies. Zirconia, for instance, is much harder than porcelain [1], but a highly polished zirconia surface can significantly reduce enamel wear on opposing teeth [1]. Interestingly, research shows that the surface finish of the material is more important than its hardness.
Highly polished zirconia has been shown to cause less wear on opposing enamel compared to glazed porcelain. The Journal of Prosthodontic Research highlights this point:
Highly polished zirconia yielded lower antagonist wear compared with porcelains. Polishing of zirconia is possible, but glazing is not recommended for the surface finish of zirconia [1].
These insights underline the importance of surface treatment when choosing materials, especially with advancements in digital fabrication.
CAD/CAM Technology Improvements
Modern CAD/CAM technology has revolutionised the way dental restorations are manufactured. Industrially produced ceramic blocks offer greater consistency and reliability compared to laboratory-processed porcelains, which are more prone to flaws like voids [4]. CAD/CAM systems use oversized "greenware" blocks to account for the approximately 30% volume shrinkage that occurs during firing [5].
The results speak for themselves. Machined feldspathic ceramics achieve fracture strengths of about 772.3 N, while zirconia crowns produced through CAD/CAM can withstand forces of approximately 1,000 N. Both far exceed the typical occlusal loads seen in daily function, which range from 150 to 665 N [4].
Additionally, innovations like rapid-layer technology allow aesthetic ceramics to be bonded to durable substrates. Monolithic designs, which eliminate the risk of veneer chipping, can sustain load capacities of 1,050 ± 120 N even after extensive cyclic loading [10]. These advancements ensure restorations are not only functional but also long-lasting and aesthetically pleasing.
sbb-itb-2be92ed
Conclusion
Key Points Summary
Porcelain and ceramic materials each bring unique benefits and challenges to the table. Feldspathic porcelains are known for their excellent aesthetics, making them ideal for anterior restorations, though they lack the strength needed for high-stress areas. On the other hand, zirconia offers superior strength and fracture resistance, but its opacity can limit its use in highly aesthetic cases [1]. Lithium disilicate strikes a balance, providing both durability and appealing aesthetics, with flexural strengths typically ranging between 300 and 400 MPa [8].
These differences underscore the importance of choosing materials based on the specific demands of each case. For posterior teeth, which endure more stress, stronger materials like zirconia or lithium disilicate are better suited. Meanwhile, glass-based ceramics are more appropriate for anterior restorations where appearance is a priority [7].
Monolithic restorations are another option to consider, as they minimise the risk of veneer chipping and are generally more reliable [2]. Additionally, CAD/CAM blocks, which are industrially manufactured, ensure greater consistency and reduce the likelihood of processing defects [1] [6].
Choosing the Right Material
Selecting the best material depends on a variety of factors, including the location of the tooth, the level of occlusal forces, aesthetic preferences, and habits such as teeth grinding. As Siamak Najafi-Abrandabadi, DDS, explains:
It is important for dentists and laboratory technicians to have a complete knowledge of the properties and characteristics of ceramics in order to select the most appropriate restorative materials for each case [11].
If you’re unsure which material is right for your needs, consulting a dental professional is crucial. For personalised guidance on cosmetic dentistry options, including porcelain veneers and dental crowns, Dr. James Hanna at Complete Smiles Bella Vista (https://completesmilesbv.com.au) can help you make the best choice for both function and aesthetics.
Dental Ceramics: Pros and Cons of Lithium Disilicate, Zirconia & More
FAQs
What’s the difference between porcelain and zirconia crowns in dentistry?
Porcelain and zirconia are two commonly chosen materials for dental crowns, each with its own strengths in terms of durability, functionality, and appearance. Zirconia, crafted from zirconium oxide, is known for its incredible strength and resistance to chipping or cracking. This makes it an excellent option for back teeth or for individuals who grind their teeth (a condition called bruxism). In contrast, porcelain is prized for its natural, translucent appearance that closely resembles real tooth enamel, making it a go-to choice for front teeth where appearance matters most.
Zirconia crowns are typically made from a single, solid piece, which gives them outstanding durability. However, they don’t naturally have the same level of translucency as porcelain. To address this, newer translucent zirconia options have been developed, offering a better balance between strength and aesthetics. Porcelain crowns, especially those fused to a metal base, provide strikingly realistic visual results, though they’re better suited for areas of the mouth that experience less biting pressure. Clinics such as Complete Smiles Bella Vista offer both zirconia and porcelain crowns, helping patients select the best material to meet their functional and aesthetic needs.
How does lithium disilicate compare to other dental ceramics in terms of strength and appearance?
Lithium disilicate offers an impressive combination of durability and visual appeal, making it a go-to material for dental restorations. With a flexural strength of about 500 MPa, it outperforms feldspathic and leucite-based porcelains in strength, though it doesn’t quite reach the levels of zirconia, which can exceed 1,250 MPa. What sets lithium disilicate apart is its tooth-like translucency and ability to match natural tooth colour, making it a standout choice for front teeth restorations where appearance is key.
Zirconia, on the other hand, is unmatched in fracture resistance, making it the preferred option for high-stress uses like long-span bridges. However, when it comes to single crowns, inlays, and onlays, lithium disilicate often takes the lead due to its natural look and dependable strength. While newer high-translucency zirconia materials have improved in appearance, they still don’t quite match the lifelike translucency of lithium disilicate. Thanks to its balance of strength and aesthetic appeal, lithium disilicate remains a reliable choice for a wide range of dental procedures.
Why is zirconia often used for dental restorations in high-stress areas of the mouth?
Zirconia has become a go-to material for dental restorations, especially in high-pressure areas like back molars. Why? Its strength and durability make it capable of handling the intense chewing forces these teeth endure. With impressive flexural strength and resistance to fractures, zirconia is built to last, even under constant stress.
What’s more, zirconia doesn’t just hold up against wear – it’s also gentle on the surrounding tissues. Its biocompatibility ensures it integrates well in the mouth, offering both safety and long-term performance. This combination of resilience and compatibility makes zirconia a trusted option for restoring both function and appearance in the toughest spots.
Related Blog Posts
- Durability of Metal-Ceramic Restorations
- Ceramic Materials in Crowns and Bridges
- Zirconia vs. Ceramic: Biocompatible Dental Materials
- Porcelain vs Lithium Disilicate: Flexural Strength Explained
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





