







Oral Epithelium: Key Cell Types Explained

The oral epithelium is a protective tissue lining your mouth, made up of three main cell types: keratinocytes, melanocytes, and Langerhans cells. Each plays a vital role in maintaining oral health:
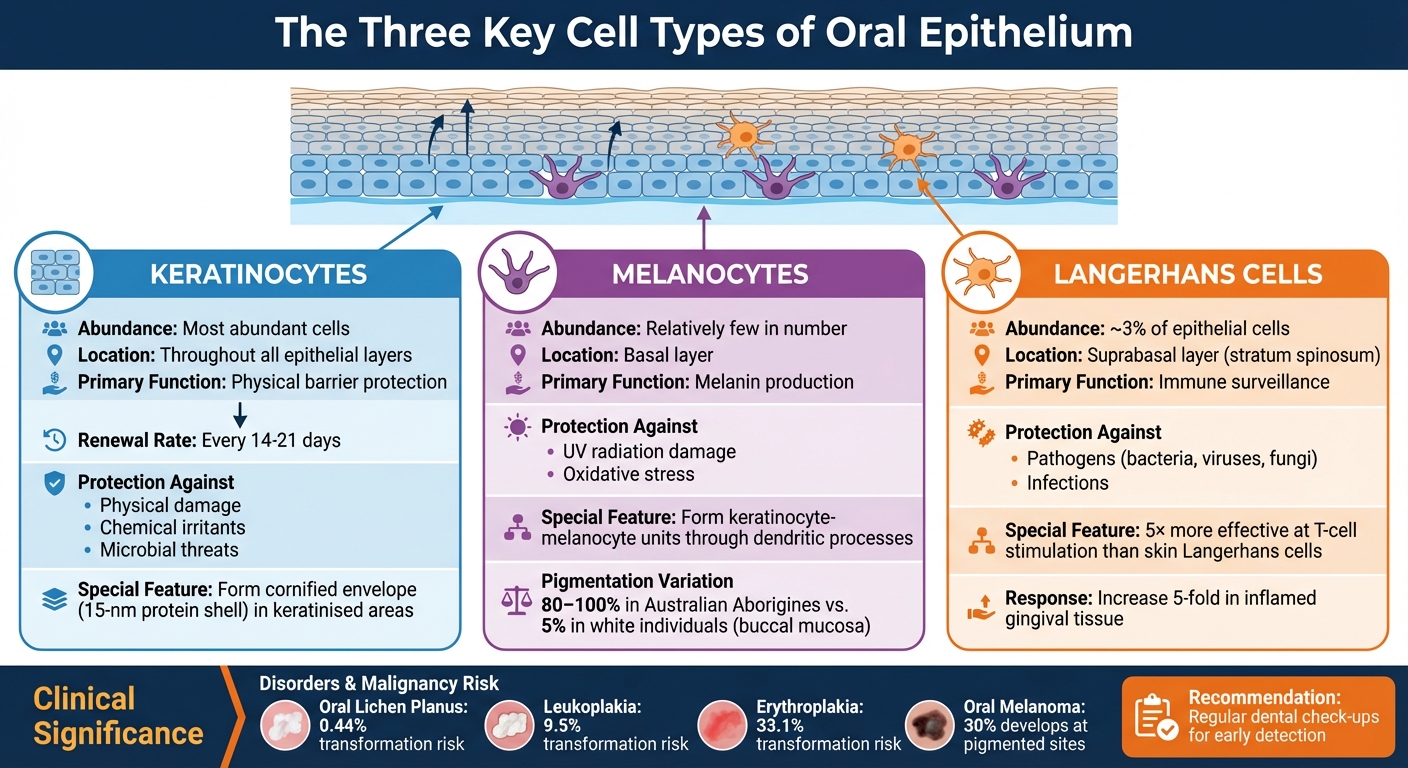
- Keratinocytes: The most abundant cells, forming a tough barrier against physical, chemical, and microbial damage. They renew every 14–21 days, keeping the mouth resilient.
- Melanocytes: Found in the basal layer, these cells produce melanin, which protects DNA from UV damage and offers antioxidant benefits.
- Langerhans cells: Immune cells in the suprabasal layer, responsible for detecting threats and activating T-cells to fight infections.
The epithelium is divided into three types:
- Masticatory mucosa (keratinised): Found on the hard palate and gums, designed for high friction areas.
- Lining mucosa (non-keratinised): Covers flexible areas like cheeks and lips, allowing movement.
- Specialised mucosa: Located on the tongue, containing taste buds.
Oral health issues like lichen planus, leukoplakia, or oral cancer often stem from disruptions in these cells. Regular dental check-ups help detect changes early, ensuring effective treatment and prevention.
Three Key Cell Types in Oral Epithelium: Functions and Locations
Oral Mucosa – Keratinized and Non-keratinized epithelium
Keratinocytes: The Primary Cell Type
Keratinocytes dominate the oral epithelium, forming a stratified squamous structure that serves as the main defence between the oral cavity and the underlying tissues [2]. These cells originate in the basal layer, where they proliferate and then migrate upwards, replacing older cells. This constant renewal is key to maintaining the epithelium’s protective role, as outlined below.
The strength of keratinocytes comes from their tonofilaments and tight desmosomal connections, with hemidesmosomes anchoring them securely to the basement membrane. This setup is crucial for shielding the oral environment.
Barrier Function
The combination of keratinocyte renewal and their structural features creates an effective barrier. Keratinocytes protect the oral mucosa from mechanical stress, chemical irritants, and microbial threats [2]. In areas with keratinised epithelium, mature keratinocytes develop a cornified envelope – a durable 15-nm protein shell reinforced by compact keratin filaments. This results in an exceptionally strong barrier, particularly in regions exposed to significant friction.
While this rapid renewal process helps prevent long-term damage, it also makes the oral epithelium more vulnerable to treatments like chemotherapy, which can result in painful oral ulcers [2].
Keratinised vs. Non-Keratinised Epithelium
The oral cavity features two types of epithelium, each adapted to its specific function. Keratinised epithelium undergoes full maturation, forming a tough outer layer called the stratum corneum. In these areas, the surface cells may be orthokeratinised (lacking nuclei) or parakeratinised (with shrunken, pyknotic nuclei) [2].
Non-keratinised epithelium, on the other hand, lines more flexible areas. Here, keratinocytes do not form a granular layer or a cornified surface. Instead, they retain their nuclei, staying moist and elastic to accommodate movements required for speech and chewing. For example, the buccal mucosa, which can measure over 500 micrometres in thickness, showcases this flexibility. Interestingly, non-keratinised regions can develop a keratin layer in response to chronic irritation, such as the formation of a linea alba from habitual chewing [2].
| Feature | Keratinised (Masticatory) Epithelium | Non-Keratinised (Lining) Epithelium |
|---|---|---|
| Primary Layers | Stratum basale, spinosum, granulosum, corneum | Stratum basale, spinosum, intermedium, superficiale |
| Surface Cells | Flat squames; may be orthokeratinised (no nuclei) or parakeratinised (pyknotic nuclei) | Squamous cells with visible, healthy nuclei |
| Granular Layer | Present (contains keratohyalin granules) | Absent |
| Function | Tough and resistant to abrasion and friction | Flexible, distensible, and mobile lining |
| Location | Hard palate, gingiva, parts of the tongue | Cheeks, lips, soft palate, floor of mouth |
| Turnover Rate | Slower (e.g. 24 days for hard palate) | Faster (e.g. 14 days for buccal mucosa) |
Melanocytes: Pigmentation Cells
Melanocytes are specialised dendritic cells found in the basal layer of the oral mucosa, responsible for producing melanin. These cells, though relatively few in number[3], play a key role in shielding oral tissues by producing melanin and contributing to immune defence mechanisms.
During embryonic development, melanocytes originate from the neural crest and migrate to the oral mucosa. Each melanocyte forms connections with nearby keratinocytes through dendritic processes, creating what is known as the keratinocyte-melanocyte unit[3]. This structure ensures efficient pigment distribution and supports their protective functions.
Melanin Production and Protection
Melanocytes synthesise melanin within specialised organelles called melanosomes through a process known as melanogenesis. This involves the oxidation of tyrosine, a reaction primarily driven by the enzyme tyrosinase[3][4]. The result is the production of two main types of melanin: eumelanin (a brown-black pigment) and pheomelanin (a yellow-red pigment). Once melanin is formed, the mature melanosomes are transferred to adjacent keratinocytes via the dendritic extensions of melanocytes. Within these keratinocytes, the melanin clusters to form supranuclear caps, offering protection to nuclear DNA from ultraviolet (UV) radiation[3].
Beyond UV defence, melanin also functions as an antioxidant. Melanosomes contain enzymes like acid phosphatase and β-galactosidase, which help break down bacteria. As keratinocytes naturally shed, this enzymatic activity enhances the oral mucosa’s physical barrier[3][4].
Differences in Oral Pigmentation
Oral pigmentation varies widely between individuals, largely due to genetic differences. Interestingly, the number of melanocytes remains relatively consistent across ethnic groups. However, the quantity and type of melanin produced can differ significantly[3][4]. For instance, physiological oral pigmentation is observed in 80% to 100% of Australian Aborigines, compared to only about 5% of white individuals who exhibit pigmentation in the buccal mucosa[3].
The gingiva is the most commonly pigmented area in the oral cavity. This pigmentation typically appears symmetrically on both sides and is limited to the attached gingiva, never extending past the mucogingival junction[3][4]. Environmental factors such as smoking, certain medications, and chronic inflammation can also influence the intensity of pigmentation. Additionally, as individuals age, both the number of melanocytes and the degree of pigmentation tend to increase. This is often due to accumulated environmental exposure and minor injuries over time[3].
sbb-itb-2be92ed
Langerhans Cells: Immune Defence Cells
Langerhans cells (LCs) play a key role in the oral immune system, complementing the protective functions of keratinocytes and melanocytes. These specialised immune cells act as sentinels, constantly monitoring for potential threats. Found primarily in the suprabasal (stratum spinosum) layer of the oral epithelium, they make up about 3% of the cell population in this tissue [21, 23, 26]. Unlike their counterparts in the skin, oral LCs are continually replenished by bone marrow–derived pre-dendritic cells and monocytes circulating in the bloodstream [22, 29].
Interestingly, oral LCs are five times more effective at stimulating T-cell proliferation than skin LCs [8]. This heightened capability is essential for distinguishing harmful pathogens from the mouth’s natural bacterial residents, reflecting their unique origin and replenishment process.
Antigen Presentation and Immune Response
Oral LCs are equipped with higher levels of TLR2 and TLR4 compared to skin LCs, enabling them to detect pathogens quickly [6]. They capture antigens into specialised structures called Birbeck granules, which have a distinct "tennis racket" shape [23, 26].
Upon activation, LCs mature and migrate through lymphatic vessels to nearby lymph nodes. There, they present antigenic peptides, bound to MHC Class II molecules, to naive CD4⁺ T-cells. This interaction triggers a targeted immune response, crucial for combating pathogens like Porphyromonas gingivalis (a major contributor to periodontitis), Candida species, and viruses such as HIV and HPV [23, 25, 26].
Protection Against Oral Pathogens
Beyond initiating immune responses, LCs help maintain a delicate balance in the oral environment by promoting tolerance to harmless commensal bacteria and food antigens [21, 25]. This balance is critical in conditions like periodontitis, where the number of LCs in inflamed gingival tissue can increase fivefold compared to healthy tissue [5].
However, LC function can be affected by various factors. Ageing, for instance, reduces their ability to migrate, which may increase vulnerability to infections and cancers [7]. Tobacco and alcohol use also impair their activity [9]. In severe cases, such as HIV-1 infection, LCs not only become targets but also serve as reservoirs for the virus, further weakening the mucosal immune defence [5].
Clinical Applications in Oral Health
The cellular makeup of the oral epithelium plays a crucial role in diagnosing and managing various oral health conditions. Changes in keratinocytes, melanocytes, and Langerhans cells can disrupt tissue structure and lead to clinical issues, from benign pigmentation changes to serious malignancies.
Disorders Related to Epithelial Cell Types
Keratinocyte-related disorders are a common cause of oral conditions. For example, oral lichen planus (OLP), which affects about 0.89% to 0.98% of people worldwide, occurs when T-cells attack basal keratinocytes. This immune response damages the basement membrane, causing cell death [10]. OLP can appear as white, net-like patterns (Wickham’s striae) or painful erosions and carries a small risk (0.44%) of becoming malignant, requiring long-term monitoring [10]. Other conditions, like leukoplakia (white patches) and erythroplakia (red patches), are more concerning, with transformation risks of 9.5% and 33.1%, respectively. Biopsies are essential to rule out dysplasia or early cancer in these cases [11].
Melanocyte disorders range from benign to life-threatening. Smoker’s melanosis, a harmless brown discolouration caused by tobacco use, often reverses after quitting [3]. However, oral mucosal melanoma, though rare, is far more serious. It can develop in about 30% of cases at sites with pre-existing pigmentation. Any sudden changes in pigmentation should be thoroughly investigated [3].
Langerhans cell dysfunction weakens immune defences in the oral mucosa. These immune cells help protect against infections, and their altered function may increase the risk of malignant transformations [9].
| Cell Type | Condition | Transformation Risk |
|---|---|---|
| Keratinocytes | Oral Lichen Planus | 0.44% [10] |
| Keratinocytes | Leukoplakia | 9.5% [11] |
| Keratinocytes | Erythroplakia | 33.1% [11] |
| Melanocytes | Oral Melanoma | Develops in 30% at pigmented sites [3] |
These conditions highlight the importance of regular clinical evaluations by dental professionals.
Role of Dental Professionals
Dental professionals play a key role in identifying and managing epithelial abnormalities. Routine oral exams should include careful checks for colour changes, such as white patches that don’t wipe off, velvety red areas, or new pigmentation. Persistent ulcers lasting over two weeks should be biopsied to rule out malignancy [12]. Techniques like bimanual palpation can detect underlying induration, while restricted mouth opening (trismus) may signal submucosal changes [12].
"The oral epithelium acts as a barrier against these physiological and pathogenic stresses. It functions as a physical and an immune barrier to external aggressions." – StatPearls [1]
Prevention is just as important as early detection. Educating patients about risk factors – like tobacco use, alcohol consumption, and poor oral hygiene – helps maintain epithelial health [11]. For conditions like OLP, topical corticosteroids such as clobetasol propionate are often the first treatment option [10]. Since oral epithelial cells regenerate every 14 to 21 days, observing healing patterns after removing irritants (e.g., sharp teeth or poorly fitting dentures) can provide valuable diagnostic clues [1][12].
In Australia, dental clinics like Complete Smiles Bella Vista (https://completesmilesbv.com.au) conduct thorough oral examinations, aiding in the early detection and effective treatment of these conditions. Ongoing attention to these issues is vital for achieving the best outcomes for patients.
Conclusion
Oral health relies on the coordinated efforts of three key cell types. Keratinocytes act as the primary structural defence, creating a physical barrier and releasing cytokines to fight off pathogens [13]. Langerhans cells serve as immune sentinels, capturing pathogens and initiating specific T-cell responses via regional lymph nodes [14]. Meanwhile, melanocytes produce melanin, offering protection against oxidative stress [6, 10].
When these cells are disrupted, oral health can suffer. For example, the breakdown of keratinocyte junctions by pathogens like P. gingivalis can trigger inflammatory conditions such as periodontitis [13]. Interestingly, the oral mucosa contains significantly more T-lymphocytes than skin, underscoring its robust immune defence [14]. Additionally, with the buccal mucosa renewing every 14 to 25 days, changes in epithelial cells may signal systemic diseases, chronic irritation, or even malignancy [2].
Given the importance of these cellular defences, even minor changes should not be ignored. Routine dental check-ups are essential for identifying shifts in keratinisation, pigmentation, or immune responses. Dental professionals should carefully screen for hyperkeratosis in areas that are typically non-keratinised and monitor unusual pigmentation changes, as these could indicate chronic irritation or the early stages of cellular abnormalities that may require a biopsy [2]. Maintaining good oral hygiene also helps to preserve the balance of the oral microbiome, protecting mucosal integrity and overall health [13].
FAQs
What do keratinocytes, melanocytes, and Langerhans cells do in the oral epithelium?
Keratinocytes, melanocytes, and Langerhans cells are crucial players in keeping the oral epithelium healthy and functional.
Keratinocytes make up the bulk of the oral epithelium. Their main job? Producing keratin to form a protective barrier. This barrier acts as a shield, safeguarding the tissues beneath from physical harm, chemical irritants, and microbial threats. Thanks to keratinocytes, the oral mucosa stays resilient and robust.
Melanocytes, on the other hand, are responsible for producing melanin – the pigment that gives oral tissues their colour. Beyond aesthetics, melanin offers protection against UV damage, playing a key role in defending sensitive tissues. These cells also explain the natural variations in oral pigmentation among different individuals.
Lastly, Langerhans cells serve as the immune system’s watchtower in the oral cavity. These specialised immune cells are on constant alert, detecting harmful pathogens and initiating immune responses. Their work is vital in preventing infections and ensuring overall oral health.
What causes variations in oral pigmentation, and what factors play a role?
Oral pigmentation varies due to differences in melanin production and how it is distributed within the oral epithelium. Melanocytes, the specialised cells found in the basal layer of the oral mucosa, are responsible for producing melanin. The amount of melanin produced is shaped by factors like genetics, racial background, and environmental influences. For example, individuals with darker skin tones tend to have more noticeable pigmentation. Interestingly, this is due to increased melanin production rather than a higher number of melanocytes.
Beyond genetic factors, hormonal changes, certain medications, or exposure to external substances – such as heavy metals or tobacco – can also affect oral pigmentation. These changes often appear as brown, black, or grey spots or lesions within the mouth. While most pigmentation is harmless and considered physiological, any significant or sudden changes should be evaluated by a dental professional to ensure there are no underlying health concerns.
What oral health problems can arise from damage to the oral epithelium?
When the oral epithelium is damaged, it can trigger a range of oral health problems, including ulcers, lesions, and a higher risk of infections. One common concern is oral mucosal diseases, which might show up as white or red patches, ulcers, or even pigmented areas. These issues can arise from trauma, infections, inflammation, or, in some cases, malignant changes in epithelial cells.
A compromised epithelium also weakens its role as a protective barrier, leaving the mouth more prone to infections like oral thrush or bacterial conditions. Inflammatory problems, such as periodontal disease, can emerge when harmful bacteria disrupt the epithelium’s immune response. Damage to critical epithelial cells – like keratinocytes, melanocytes, or Langerhans cells – can slow healing and weaken immune defences, further jeopardising oral health.
Taking care of the oral epithelium is crucial for protecting against these challenges and maintaining overall oral health.
Related Blog Posts
- When Should Smokers Get Oral Cancer Screening?
- Early Signs of Smoking-Related Oral Cancer
- Diabetes and Periodontitis: Oral Microbiome Changes
- Differential Diagnosis for Periodontal Infections
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





