







Differential Diagnosis for Periodontal Infections

Periodontal infections, ranging from mild gingivitis to severe periodontitis, can silently progress and lead to significant oral and systemic health issues. Misdiagnosis is common as other conditions, like pulpal problems or systemic diseases, often mimic these infections. Accurate diagnosis is vital because:
- Early symptoms are subtle: Redness, swelling, or bleeding may go unnoticed.
- Systemic links are strong: Conditions like diabetes and cardiovascular disease are often connected to periodontal health.
- Misdiagnosis delays treatment: Some symptoms may indicate broader health problems, such as immune disorders or infections.
Key types of periodontal infections include plaque-related (caused by bacterial biofilm) and non-plaque conditions (linked to systemic or immune issues). Proper diagnosis involves detailed medical history, clinical exams, imaging, and sometimes biopsies or blood tests. Clinics like Complete Smiles Bella Vista integrate screenings into routine check-ups for early detection and tailored care.
Treatment varies by diagnosis, from scaling and antimicrobial therapy for plaque-related cases to multidisciplinary approaches for systemic conditions. Early intervention prevents complications like tooth loss and supports overall health.
The Only Way To Diagnose Gum Disease – New BSP classification made easy
Types of Periodontal Infections
Periodontal infections can be grouped into two main categories: plaque-related periodontal diseases and non-plaque periodontal conditions. Plaque-related diseases are primarily caused by the buildup of bacterial biofilm, which triggers inflammation that can progress from reversible gingivitis to destructive periodontitis. On the other hand, non-plaque conditions arise from factors like systemic illnesses, immune dysfunction, specific pathogens (such as viruses or fungi), trauma, or genetic predisposition. In these cases, plaque may play a secondary role, exacerbating the condition rather than being the primary cause [3].
Plaque-related diseases often develop gradually and are closely tied to oral hygiene habits. Non-plaque conditions, however, tend to show unusual patterns, such as rapid onset, disproportionate pain, systemic symptoms, or resistance to standard treatments like scaling and home care [1]. A clear understanding of these categories is essential for accurate diagnosis, as outlined in the following sections.
Plaque-Related Periodontal Diseases
Gingivitis is the most common and earliest form of plaque-related disease. It presents as red, swollen gums that bleed easily during brushing or probing. Importantly, there is no loss of attachment or bone at this stage, and the inflammation is confined to the gingiva. With proper plaque control, such as regular brushing, flossing, and professional cleaning, gingivitis is entirely reversible. Clinically, the gums may appear swollen, tender, and covered with visible plaque deposits.
If gingivitis is not addressed, it can progress to periodontitis. In this stage, the body’s immune response to the bacterial biofilm becomes dysregulated, leading to destruction of the periodontal ligament and alveolar bone [4]. This results in attachment loss, periodontal pockets deeper than 3 mm, gum recession, and, in severe cases, tooth mobility or loss. Radiographs may show bone loss, and patients might notice persistent bad breath, shifting teeth, or even abscesses.
In Australia, dental practitioners use the 2018 World Workshop staging and grading system, endorsed by the Australian Dental Association in 2021, to classify periodontitis based on its severity and rate of progression. This system helps tailor treatment plans and determine follow-up intervals.
The primary culprit in plaque-related diseases is the dental plaque biofilm, which hosts harmful bacteria like Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans. Several factors can influence the progression from gingivitis to periodontitis, including smoking, poorly controlled diabetes, genetic predisposition, and stress. In Australia, specific challenges – such as high smoking rates in some communities, an ageing population, increasing cases of type 2 diabetes, and limited access to dental care in rural areas – can allow these diseases to worsen before treatment is sought.
In contrast, non-plaque conditions often require more specialised diagnostic approaches due to their atypical presentations.
Non-Plaque Periodontal Conditions
Non-plaque conditions stem from systemic issues, immune dysfunction, trauma, or genetic factors. One example is necrotising periodontal diseases, which include necrotising gingivitis, necrotising periodontitis, and necrotising stomatitis. These conditions are characterised by punched-out interdental papillae covered with a grey pseudomembrane, spontaneous bleeding, and a foul odour [1]. They are more common in individuals who are immunocompromised, malnourished, under high stress, or heavy smokers. Treatment typically involves urgent debridement, antimicrobial rinses, systemic antibiotics, and addressing underlying nutritional or immune deficiencies.
Certain infections – whether bacterial, viral, or fungal – can also mimic plaque-related periodontal diseases. For instance, conditions like syphilis, tuberculosis, gonorrhoea, herpes simplex, varicella zoster, candidiasis, or histoplasmosis may cause ulcerations, granulomas, vesicles, or necrotic tissue. These often occur in unusual locations or are accompanied by systemic symptoms like fever. Such cases usually require further diagnostic tests, such as microbiological cultures or biopsies, to confirm the cause.
Immune-mediated and systemic diseases can also affect periodontal tissues. Conditions like oral lichen planus, mucous membrane pemphigoid, pemphigus vulgaris, and graft-versus-host disease often present as desquamative gingivitis, with symptoms including diffuse redness, peeling epithelium, and pain even with minor trauma. These conditions may also involve other areas of the body. Patients with autoimmune disorders, blood-related conditions (like leukaemia), or rare genetic syndromes (such as Papillon–Lefèvre or Down syndrome) need careful evaluation, as improving plaque control alone is usually insufficient. Targeted medical treatment is often necessary.
Non-plaque conditions frequently exhibit unusual features, such as sharply defined lesions that don’t align with plaque distribution, vesicles, bullae, necrosis, or white striae. They are also more likely to cause significant discomfort or burning sensations. When these conditions don’t respond to standard plaque control measures, further investigations – like detailed medical histories, biopsies, microbiological tests, and blood work – are essential. Referral to specialists is often required to ensure accurate diagnosis and effective treatment.
Conditions That Resemble Periodontal Infections
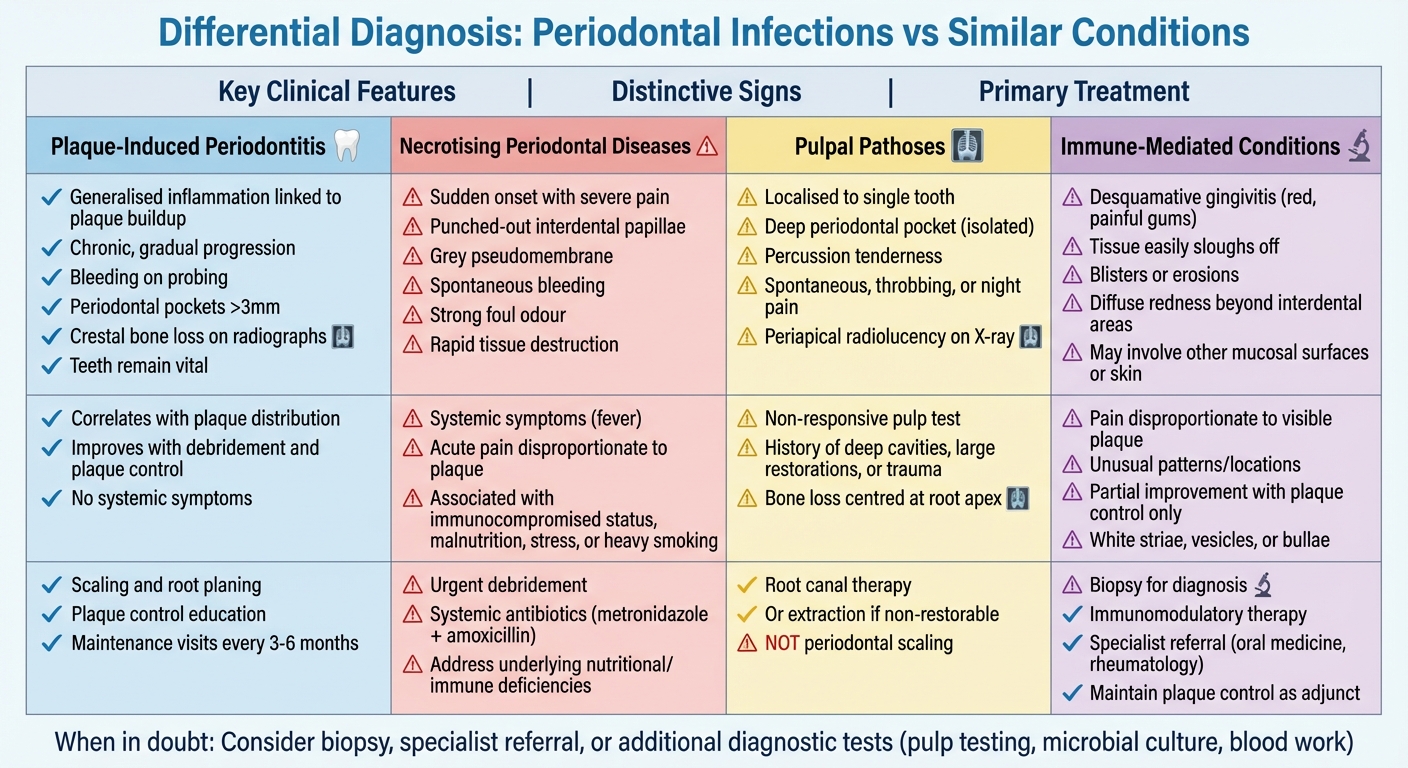
Differential Diagnosis Guide for Periodontal Infections vs Similar Conditions
Some conditions can look like periodontal infections, making it harder to diagnose them correctly. These issues might cause gum swelling, bleeding, pain, or even tissue destruction, but their causes aren’t related to plaque-induced periodontitis. Spotting these conditions early is crucial to avoid the wrong treatments and ensure patients get the care they need. Understanding these conditions plays a key role in refining diagnostic methods, which will be discussed in the next section.
Necrotising Periodontal Diseases
Necrotising periodontal diseases are distinct from typical plaque-related conditions due to their sudden onset, severe pain, and rapid tissue destruction. This group includes necrotising gingivitis, necrotising periodontitis, and necrotising stomatitis. They are characterised by cratered papillae, a greyish pseudomembrane, spontaneous bleeding, and a strong foul odour. Systemic symptoms like fever often accompany these conditions [1].
The severity of tissue involvement sets these conditions apart. Necrotising gingivitis primarily affects the interdental papillae and marginal gingiva, with minimal attachment loss. Necrotising periodontitis, on the other hand, involves rapid attachment and bone loss around affected teeth. Necrotising stomatitis goes beyond the gums, affecting adjacent oral tissues and sometimes exposing the underlying bone [1]. These conditions are often misdiagnosed as "severe gum infections" because clinicians might focus on bleeding and bad breath without recognising necrotic papillae, acute pain, or relevant predisposing factors [1][3]. For instance, a young adult in Sydney undergoing chemotherapy might present with severe pain, cratered papillae between the lower incisors, a pseudomembrane, and fever. In such cases, what might initially seem like "acute periodontitis" could actually be necrotising periodontitis, requiring immediate debridement, systemic antibiotics, and collaboration with the patient’s medical team.
Pulpal Pathoses
Pulpal conditions like acute apical abscesses, chronic apical periodontitis, and endo-perio lesions can mimic localised periodontitis. These conditions often present with deep periodontal pockets, localised swelling, pus, and radiographic bone loss [2]. The key difference lies in the tooth’s vitality and the bone loss pattern. Indicators include a history of deep cavities, large restorations, or trauma; pain that is spontaneous, throbbing, or occurs at night (pointing to a pulpal origin) rather than dull discomfort during chewing; and a non-responsive pulp test in endodontic cases [2]. Radiographs typically show a periapical radiolucency centred at the root apex, which may extend coronally along the root, unlike the generalised crestal bone loss seen in periodontal disease.
Misdiagnosing these conditions can lead to unnecessary periodontal treatments like surgery or scaling when root canal therapy or extraction is actually required. Clinics like Complete Smiles Bella Vista often rely on a combination of periodontal charting, pulp testing, and periapical radiographs to determine the correct diagnosis before proceeding with treatment. These challenges highlight the importance of distinguishing pulpal issues from true periodontal infections.
Systemic and Immune-Related Conditions
Systemic infections can also mimic aggressive periodontal disease, presenting with symptoms like gingival ulceration, atypical necrosis, non-healing lesions, or granulomatous swelling. These areas may become colonised by plaque, further complicating diagnosis [1][3]. Warning signs include ulcers that don’t heal after standard periodontal therapy, unexplained weight loss, night sweats, high-risk sexual history, or travel to regions with high rates of tuberculosis. In Australia, where tuberculosis and syphilis are more common in certain migrant and remote Indigenous communities, clinicians should consider these infections when lesions are unilateral, firm, or linked to systemic symptoms. Prompt referral for medical testing or biopsy is often more appropriate than repeated deep cleaning.
Immune-related conditions like pemphigus vulgaris, mucous membrane pemphigoid, and oral lichen planus can appear as desquamative gingivitis. This condition causes red, painful gums where the outer layer of tissue easily sloughs off and bleeds. It may also involve blisters or erosions [3]. While these lesions might initially look like severe plaque-induced gingivitis, they often cause pain disproportionate to the visible plaque, affect areas beyond the interdental papillae, and may be linked to lesions on other mucosal surfaces or the skin. Lesions that show unusual patterns, disproportionate pain, or atypical locations should be biopsied and referred to specialists rather than being managed with scaling alone [3].
In some cases, plaque-induced inflammation can worsen lesions caused by systemic or immune conditions, making them look like severe periodontitis. If thorough plaque control and debridement lead to only partial improvement or reveal unusual colours, textures, or ulceration patterns, clinicians should consider non-plaque-related causes. Identifying these overlapping signs is crucial for moving forward with advanced diagnostic methods, which are explored in the next section.
sbb-itb-2be92ed
How to Diagnose Periodontal Infections
Accurate diagnosis of periodontal infections relies on a combination of patient history, clinical examination, and imaging. This approach helps distinguish true periodontal infections from other conditions that may mimic them. When assessing a patient, it’s critical to prioritise urgent symptoms such as fever, facial swelling, or severe pain, as these may require immediate intervention [5].
Patient History and Clinical Examination
A thorough medical and dental history is the cornerstone of diagnosis. It’s essential to document any systemic conditions – like diabetes, haematological disorders, or immunosuppression – that could affect periodontal health. Additionally, certain medications, such as calcium channel blockers, phenytoin, or specific immunosuppressants, are known to cause gingival overgrowth and must be considered [3]. Understanding the onset, duration, and progression of symptoms can help differentiate chronic plaque-related conditions from acute issues. For instance, sudden pain with systemic symptoms may point to necrotising periodontal disease, while a slow, gradual progression is more typical of periodontitis [1]. Lifestyle factors like smoking, alcohol consumption, stress, and poor nutrition also play a role in how the disease manifests [1].
A full-mouth charting, with probing at six sites per tooth, provides a detailed clinical picture. Key assessments include bleeding on probing, signs of suppuration, furcation involvement, recession, tooth mobility, and mucogingival defects. Visual inspections focus on plaque and calculus buildup, gingival colour and contour, and any unusual features like ulceration or pseudomembranes. Patterns of findings are crucial – extensive deep pockets with heavy plaque suggest periodontitis, whereas an isolated deep pocket on a single, thermally sensitive tooth may indicate endodontic issues. Comprehensive charting systems and digital records help track these findings and monitor disease progression over time.
These findings set the stage for further imaging and diagnostic tests as needed.
Diagnostic Tests and Imaging
Radiographic imaging is a key tool in confirming clinical observations and identifying patterns of bone loss. Bitewing, periapical, or panoramic radiographs can reveal horizontal or angular bone loss typical of chronic periodontitis, or periapical radiolucencies associated with endodontic lesions [2][6]. Combined endodontic-periodontal lesions often display a mix of features, such as vertical bone loss alongside periapical radiolucency.
When clinical and radiographic findings don’t align with expected patterns, additional tests can clarify the diagnosis. Pulp vitality testing, for example, helps differentiate primary endodontic disease from periodontal conditions [2]. In cases of rapidly progressing or treatment-resistant disease, microbial testing may be useful, though it is not routinely performed. Biopsies and medical referrals are crucial when lesions fail to respond to standard treatments, when gingival enlargement seems excessive compared to plaque levels, or when systemic symptoms suggest underlying haematological or immune-related conditions [3]. Blood tests may also reveal conditions like diabetes or haematological malignancies that could explain atypical presentations.
These diagnostic tools provide a framework for comparing clinical features across different conditions.
Comparing Different Conditions
A systematic comparison of clinical features is essential for accurate differential diagnosis. Plaque-induced periodontitis typically shows generalised inflammation linked to plaque buildup, follows a chronic course, and involves teeth that remain vital. Necrotising periodontal diseases, on the other hand, are marked by distinct signs such as punched-out interdental papillae, grey pseudomembranes, spontaneous bleeding, and severe pain, often accompanied by systemic symptoms [1]. Pulpal pathoses usually affect a single tooth, presenting as a localised deep pocket with percussion tenderness and altered pulp vitality [2]. Immune-mediated conditions might cause widespread gingival redness, mucosal sloughing, and pain that seems disproportionate to the amount of plaque present [3].
Monitoring the response to treatment is also vital. Periodontal infections typically improve with debridement and plaque control, while persistent lesions may indicate a non-plaque-related cause that requires a different approach. The 2017 World Workshop classification system provides further guidance by categorising periodontal conditions based on staging (severity and complexity) and grading (rate of progression, systemic risk factors, and radiographic bone loss relative to age). This framework aids in both diagnosis and treatment planning [6].
Treatment Options Based on Diagnosis
Once a diagnosis is confirmed, treatment plans should be tailored to address the specific condition. For plaque-related periodontal infections, mechanical and antimicrobial strategies work effectively, while systemic or immune-related cases often call for a team approach involving medical specialists. The treatment approach must align with the root cause of the issue.
Treating Periodontal Infections
For plaque-induced conditions, the primary focus is on controlling plaque. This starts with educating patients on proper oral hygiene practices, such as brushing twice daily with a soft-bristled toothbrush, flossing daily, and, when recommended, using antimicrobial rinses like chlorhexidine. Professional scaling and root planing is a key non-surgical treatment that removes plaque below the gumline and smooths root surfaces. This process can reduce inflammation and decrease pocket depths by 1–2 mm on average. When combined with maintenance visits every three to six months, non-surgical therapy successfully halts disease progression in 80–90% of cases [4][6].
Antimicrobial therapy may be necessary for persistent infections or deeper periodontal pockets (5–7 mm) that do not respond adequately to scaling alone. Localised antimicrobial agents, such as minocycline microspheres, can be applied directly into the pockets, while systemic antibiotics like amoxicillin or metronidazole are used to target aggressive pathogens such as Porphyromonas gingivalis. Research shows that adjunctive antimicrobial treatments can improve clinical outcomes by 20–40% in randomised trials. However, addressing risk factors like smoking is equally important for long-term success [1][4]. For necrotising periodontal diseases, treatment includes removing necrotic tissue, managing pain, and administering systemic antibiotics (such as metronidazole combined with amoxicillin for 7 days), while also addressing underlying factors like malnutrition or stress [1].
In more advanced cases, surgical interventions such as flap surgery or bone grafting may be required, especially when non-surgical methods fail to yield results. Early treatment can prevent tooth loss and other complications, but success hinges on the patient’s commitment to maintaining good oral hygiene at home [6][7].
Managing Systemic and Complex Cases
For cases where systemic conditions or treatment resistance complicate periodontal health – such as diabetes, HIV, or autoimmune disorders – a multidisciplinary approach is crucial. Patients with diabetes, for instance, are two to three times more likely to develop severe periodontitis. Coordinated care between dental and medical professionals can help reduce systemic inflammation, benefiting both oral and overall health [6]. Referral to specialists such as physicians, oral medicine experts, or haematologists is essential when systemic issues or persistent deep pockets are present [1][3][6].
For conditions like desquamative gingivitis (e.g., lichen planus), treatment focuses on controlling immune dysregulation through immunomodulatory therapies, while also maintaining plaque control to minimise additional inflammation [1][3]. Localised pulpal lesions may require root canal treatment or extraction to avoid misdiagnosis as periodontitis [2]. In cases where malignancies are suspected, biopsy-confirmed treatments – such as surgical excision, radiation, or chemotherapy – are critical. Accurate diagnosis is essential to prevent ineffective interventions like unnecessary scaling [1][2].
A collaborative approach often yields the best results. Dental practitioners may need to work closely with rheumatologists, endocrinologists, or oncologists, depending on the complexity of the case. Long-term care involves risk-based supportive periodontal therapy, guided by the 2018 staging and grading system, which tracks disease progression using metrics like bone loss relative to age. Addressing modifiable risk factors, such as quitting smoking, can improve treatment outcomes by up to 50%, underscoring the importance of lifestyle changes alongside clinical care [1][4].
Conclusion
Accurate diagnosis is the cornerstone of effective treatment, particularly when distinguishing between plaque-related infections, necrotising diseases, pulpal issues, and systemic conditions. Identifying the root cause ensures that treatment focuses on addressing the problem itself, not just alleviating symptoms. A careful diagnostic process reduces the risk of misdiagnosis and prevents unnecessary treatments, underscoring the importance of differentiating periodontal infections from conditions with similar presentations.
The 2018 World Workshop Classification System offers a modern approach to categorising periodontal disease. By evaluating factors like bone loss, inflammation, and individual risk factors, this framework supports both diagnosis and treatment planning. It enables tailored care that not only addresses the infection but also considers the patient’s overall health and contributing factors.
Early diagnosis is critical. Conditions like gingivitis, when caught early and managed with proper oral hygiene and professional care, can be reversed – preventing progression to periodontitis and avoiding more serious dental complications [6].
For more complex cases, especially those involving systemic or immune-related disorders, a multidisciplinary approach becomes essential. Collaboration between specialists ensures comprehensive care that addresses both oral and systemic health.
Specialist clinics, such as Complete Smiles Bella Vista (https://completesmilesbv.com.au), play a key role in delivering advanced treatments. From root canal therapy to complex periodontal care, these practices are equipped to provide the specialised interventions that precise diagnoses demand. By focusing on accurate diagnosis and patient education, dental professionals empower individuals to maintain their oral health and prevent complications that can impact overall well-being.
FAQs
How do plaque-related periodontal diseases differ from non-plaque periodontal diseases?
Plaque-related periodontal diseases stem from the accumulation of bacterial plaque. This build-up leads to inflammation, which can harm the gums and the structures that support the teeth. Thankfully, these conditions can typically be controlled with regular oral hygiene practices and routine visits to the dentist.
In contrast, non-plaque periodontal diseases have different origins. They may be linked to genetic factors, systemic health issues like diabetes or autoimmune disorders, or specific local irritants. Since these conditions aren’t directly tied to plaque, they often demand a more targeted approach for diagnosis and treatment, focusing on addressing the root cause.
How do systemic conditions impact periodontal health?
Systemic conditions like diabetes, cardiovascular disease, and immune system disorders can have a big impact on the health of your gums. These issues can weaken your immune system, making it tougher for your body to fight infections and heal properly from gum-related problems.
Take diabetes, for instance – it can cause increased inflammation in the gums and slow down healing. Similarly, a suppressed immune system makes it easier for bacteria to cause infections. Keeping these conditions under control is a key step in protecting your oral health and avoiding complications from gum infections.
How are periodontal infections accurately diagnosed?
Diagnosing periodontal infections requires a thorough and methodical approach to ensure precision. It typically begins with a clinical examination, where your dentist looks for signs like gum inflammation, bleeding, or unusually deep periodontal pockets. To get a clearer picture, X-rays are often used to evaluate bone levels and identify any bone loss. In certain cases, microbial testing can be conducted to pinpoint the specific bacteria causing the issue.
Your dentist will also take a close look at your medical and dental history, factoring in elements like smoking, diabetes, or even a family history of gum disease that might increase your risk. Regular follow-ups are critical, as they help monitor any changes and assess how well treatments are working. Catching the problem early and diagnosing it accurately plays a big role in managing the condition and improving overall oral health.
Related Blog Posts
- 5 Early Signs of Gum Disease
- Diabetes and Periodontitis: Oral Microbiome Changes
- Periodontal Disease in Lupus Patients: Key Facts
- Flap Surgery vs. Non-Surgical Options
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





