







Machine Learning Models for Periodontal Disease

Periodontal disease affects the tissues supporting teeth and is linked to serious health issues like diabetes and cardiovascular diseases. Traditional diagnostic methods often lack precision, but machine learning is offering new tools to improve detection and management. Here’s a quick summary of how AI is transforming periodontal care:
- Early Detection: AI models analyse clinical data, imaging, and biomarkers to predict disease progression with high accuracy. For example, deep learning models like YOLOv8 achieve precision rates of 94–97% in identifying bone loss on radiographs.
- Improved Diagnosis: Logistic Regression, Random Forest, and ensemble methods classify disease types and assess risk factors like anxiety or smoking. Some models have reached 100% accuracy in specific diagnostic tasks.
- Personalised Care: AI tools help tailor treatment plans, identifying patients needing more frequent care or predicting tooth retention outcomes. For instance, models using salivary biomarkers achieved an AUROC of 0.88 for predicting disease progression.
- Challenges: Data inconsistencies, lack of standardised guidelines, and limited interpretability of AI outputs remain barriers to widespread adoption.
AI in periodontal care offers promising results but requires clinician oversight, standardised data, and ethical safeguards to ensure safe and effective use in Australian dentistry.
Dental AI: The Artificial Intelligence Revolution in Dentistry
sbb-itb-2be92ed
Machine Learning Methods Used in Periodontal Research
Researchers are leveraging various machine learning models to predict periodontal disease by analysing clinical, biological, and imaging data. The choice of model often depends on the type of data being studied – structured clinical records, biological samples, or complex imaging data. These methods range from straightforward models to ensemble approaches and advanced deep learning systems, each designed for specific diagnostic tasks.
Logistic Regression and Decision Trees
Simple supervised models like Logistic Regression and Decision Trees are highly effective for structured data, such as blood counts, probing depths, and demographic information. These models are particularly useful for categorising disease types, such as distinguishing between aggressive and chronic periodontitis. For instance, a 2023 study by Lakshmi and Dheeba involving 1,000 periodontitis patients found that Logistic Regression and Random Forest achieved 100% accuracy in classifying chronic localised versus generalised periodontitis, while Decision Trees reached 99%, with certain diagnostic tasks showing accuracies up to 98% [5][3]. One of the key benefits of these models is their interpretability, allowing clinicians to easily understand the logic behind the predictions. This clarity supports timely and targeted interventions in periodontal care. For more complex datasets, ensemble methods build on these models to deliver even greater accuracy.
Random Forest and Ensemble Learning
Ensemble methods like Random Forest and XGBoost combine multiple decision models to enhance accuracy and minimise overfitting. These techniques are particularly effective for analysing intricate datasets, such as Electronic Dental Records or non-invasive biomarkers. For example, in October 2022, researchers at Temple University applied the XGBoost algorithm to data from 27,138 dental patients, analysing 74 features, including social factors like anxiety and bruxism. This approach achieved an average Area Under the Curve (AUC) of 0.72 when differentiating between healthy, mild, and severe periodontal disease [7]. Additionally, machine learning models applied to salivary biomarkers demonstrated a pooled AUC of 0.94, outperforming models using gingival crevicular fluid, which had an AUC of 0.89. These results highlight the potential for more precise risk assessments in clinical settings [6].
Deep Learning Models
Deep learning models, such as Convolutional Neural Networks (CNNs), have become the leading choice for analysing radiographic images. Unlike traditional methods that rely on manual feature selection, these models automatically identify key features, such as alveolar bone loss or the cemento-enamel junction, directly from X-rays. Between 2018 and 2024, the Department of Oral and Maxillofacial Surgery at the University of Medicine and Pharmacy at Ho Chi Minh City developed a YOLOv8-based framework using 500 panoramic radiographs. By integrating automated bone loss measurements with patient data like age, smoking status, and diabetes, the system achieved precision and recall rates between 0.94 and 0.97 [2]. In another study, a deep learning ensemble model combining YOLOv8, Mask R-CNN, and TransUNet analysed 8,462 teeth from 320 patients, achieving a diagnostic accuracy of 89.45%. These advancements pave the way for earlier detection and more precise interventions in periodontal care [8].
As Mohammed Jafer et al. observed:
Traditional machine learning models such as SVMs and decision trees exhibited superior performances with clean, structured numerical data, but deep learning techniques thrived alone with extensive, well-annotated imaging datasets [3].
Recent Studies on Machine Learning for Periodontal Disease
Predicting Molar Loss and Tooth Retention
Between January 2015 and December 2023, researchers at Fang Hospital in Chiang Mai, Thailand, developed a model based on YOLOv8 to predict the prognosis of individual teeth. Using 2,000 panoramic radiographs, the system achieved an impressive 98% accuracy in segmenting the cemento-enamel junction and alveolar bone levels. This allowed for precise quantification of bone loss, helping guide decisions on tooth retention or extraction in line with Thai Association of Periodontology guidelines [9]. Instead of just detecting issues, this approach focuses on personalised prognosis, providing a more tailored basis for clinical decisions. These advancements in image segmentation are laying the groundwork for more comprehensive analyses of clinical risk factors.
Identifying Risk Factors for Disease Progression
Advances in imaging have also led to better identification of risk factors for periodontal disease progression. From January 2017 to August 2021, researchers at Temple University Kornberg School of Dentistry analysed electronic dental records from 27,138 patients using an XGBoost model. This study examined 74 features and achieved an average AUC of 0.72 in distinguishing between healthy, mild, and severe disease [7]. Beyond traditional indicators, the model highlighted modifiable risk factors like patient anxiety, recreational drug use, bruxism, and systemic conditions such as osteoporosis and gastrointestinal disorders.
In another study, researchers used Probabilistic Graphical Models (PGM) to integrate clinical measures, salivary IL-1β levels, age, and sex. This approach achieved an AUROC of 0.88 for predicting 12-month disease progression, significantly outperforming traditional Logistic Regression models, which reached only 0.72 [10]. As noted by Camila Pinheiro Furquim and her team:
Integrating clinical and biological information could enhance model performance compared to more simplistic approaches and potentially contribute to the development of more effective, personalised strategies [10].
This integration of diverse data sources opens new possibilities for AI applications in oral health care.
AI Applications for Oral Health Challenges
The HC-Net+ deep learning model has demonstrated diagnostic capabilities that surpass human performance in detecting stage II–IV periodontitis. In multicentre trials, HC-Net+ achieved an AUROC of 94.2%, significantly outperforming the 85.6% accuracy of periodontal specialists (p < 0.01) [4]. Notably, the use of AI assistance improved the diagnostic accuracy of junior dentists and students, enabling them to reach the performance level of experienced specialists. The model maintained over 92.4% diagnostic accuracy globally, showcasing its adaptability across different settings [4].
These findings are particularly relevant to Australian dental practices, where AI-driven tools could help address workforce shortages and improve access to specialist-level diagnostics, especially in regional areas. Research from Nihon University‘s Department of Periodontology also highlighted the value of combining socioeconomic factors – such as income, education, and employment status – with clinical data. This approach proved more effective at predicting tooth loss than relying on clinical predictors alone [11]. Together, these studies underline the growing role of machine learning in advancing personalised periodontal care and addressing broader oral health challenges in Australia.
Model Performance and Limitations
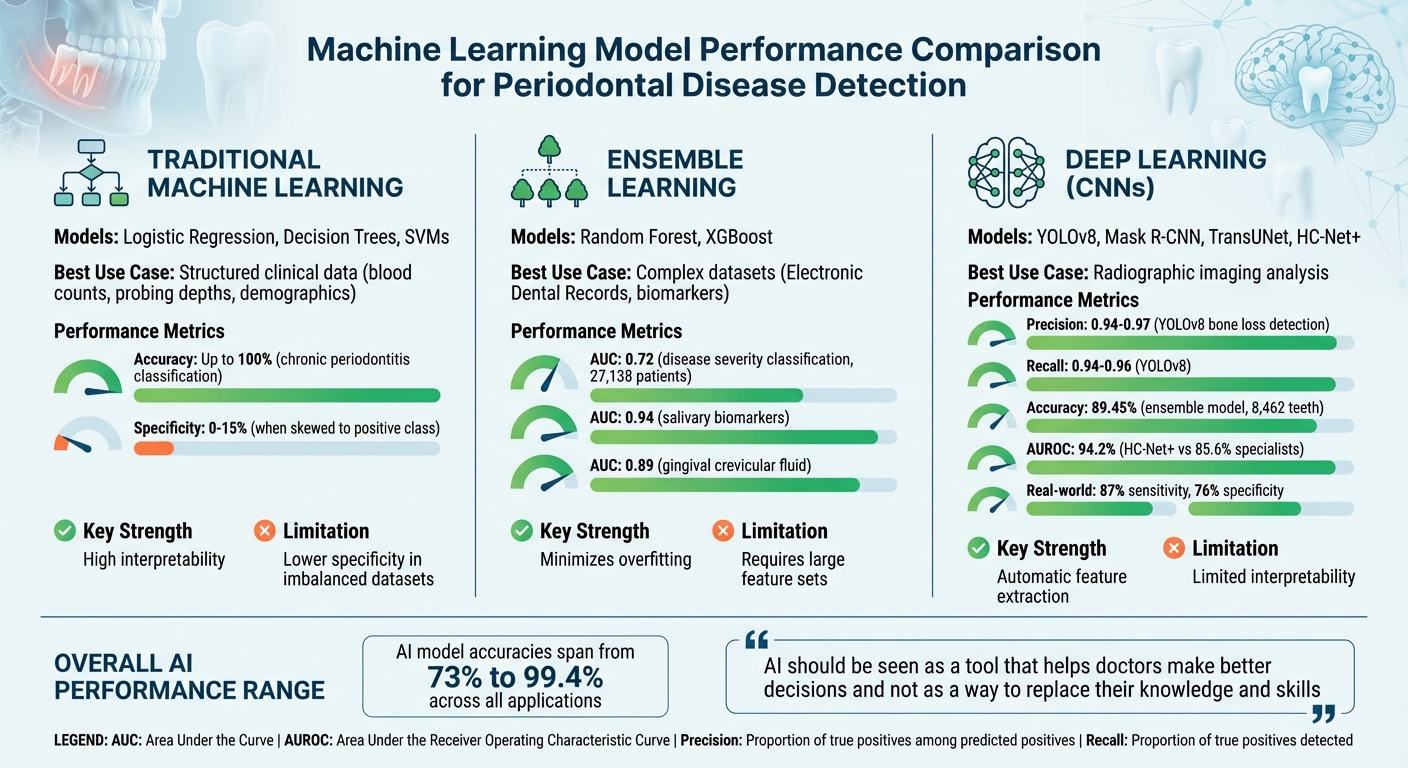
Machine Learning Model Performance Comparison for Periodontal Disease Detection
Performance Metrics Comparison
Machine learning models for periodontal disease show a wide range of performance outcomes, depending on the type of data they process. Traditional models like Logistic Regression and Support Vector Machines (SVMs) excel when working with structured clinical data. For instance, one study reported an impressive 100% accuracy in distinguishing chronic localised from generalised periodontitis, setting a high benchmark for these methods [5]. However, these models often falter in specificity, with some scoring as low as 0% to 15% when skewed towards the positive class [10].
Deep learning models, on the other hand, shine when applied to imaging datasets. A YOLOv8-based framework, for example, achieved precision rates between 0.95 and 0.97, along with recall scores of 0.94 to 0.96, for detecting bone levels and the cemento-enamel junction on panoramic radiographs [2]. Yet, real-world performance tends to be more modest. Systematic reviews indicate that AI-assisted detection of periodontal bone loss achieves around 87% sensitivity and 76% specificity [1]. Overall, AI model accuracies span from 73% to 99.4% [3].
Probabilistic Graphical Models strike a balance between these approaches. By blending clinical measures with salivary biomarkers, they achieved an AUROC of 0.88, outperforming Logistic Regression’s AUROC of 0.72 [10]. As Mohammed Jafer and colleagues emphasise:
AI should be seen as a tool that helps doctors make better decisions and not as a way to replace their knowledge and skills [3].
This point is crucial, especially since models are highly effective at identifying healthy sites (95% accuracy) but often struggle with diseased sites due to data imbalances [12]. Despite these promising results, issues with data standardisation remain a significant barrier to broader applicability.
Data Standardisation Challenges
One critical limitation affecting model performance is the lack of consistent and standardised datasets. Clinical parameters like probing depth and clinical attachment level are inherently operator-dependent, introducing variability. Similarly, radiographic quality can differ widely depending on the imaging equipment and acquisition protocols used, making it hard for models trained on one dataset to function well in different clinical environments [1][13].
Electronic dental records often miss key indicators, such as plaque index or smoking status, necessitating complex automated phenotyping before the data can be effectively used in machine learning [7]. Moreover, non-standardised case definitions and varying classification systems (e.g., AAP 1999 versus AAP 2017 guidelines) further undermine model consistency and reliability [1]. Researchers from Frontiers in Dental Medicine highlight this issue:
The limited interpretability of many deep learning models may hinder clinician trust and complicate accountability in clinical decision-making [1].
These challenges explain why models that perform well in controlled, retrospective studies often fail to generalise effectively in Australian dental practices, where equipment and patient demographics can vary significantly [13].
Clinical Applications and Future Developments
Personalised Treatment Plans
Machine learning is reshaping periodontology by enabling treatment plans tailored to individual needs. Instead of sticking to a one-size-fits-all maintenance schedule, predictive models now combine clinical data, radiographic images, and biological markers to identify patients who may require more intensive care and those who can safely extend recall intervals [1].
For example, models analysing salivary biomarkers like IL-1β and MMP-8 have achieved an AUROC of 0.88 in predicting disease progression, outperforming traditional logistic regression models, which scored 0.72 [10]. Similarly, automated systems using tools like YOLOv8 can assess panoramic radiographs in real time to measure alveolar bone loss. This not only speeds up the staging of periodontitis but also increases diagnostic accuracy. One study found AI accuracy at 94.4%, compared to 91.1% for periodontists and 86.7% for general practitioners [14].
AI is also proving useful in focusing on short-term outcomes, such as pocket depth reduction. By helping clinicians stratify periodontal sites and estimate the likelihood of improvement after non-surgical therapy, these tools enhance decision-making precision [1][12].
Requirements for Australian Dentistry
For these advanced tools to be implemented in Australia, dental practices must meet specific infrastructure and regulatory requirements. The Australian Dental Association (ADA) underscores that patient safety must come first in any AI application [15]. Importantly, AI systems cannot operate independently or be actioned directly by patients – they must always be supervised by a registered dental practitioner [15].
Practices will need to invest in advanced digital imaging technologies, secure IT systems, and data storage solutions that align with the Office of the Australian Information Commissioner (OAIC) guidelines [1][15]. Using standardised classification frameworks, such as the 2017 AAP/EFP periodontal case definitions, ensures consistent and reliable results across clinical settings [1][2].
Another critical factor is clinician training. Dentists must engage in ongoing professional development to interpret AI outputs accurately and understand their limitations. The ADA emphasises that AI should serve as a decision-support tool, supplementing – not replacing – clinical expertise [1]. Additionally, manufacturers are responsible for the information their AI systems provide, and third parties, such as insurers, are prohibited from using AI-generated data to limit patient access to appropriate care [15].
Ethical Considerations and Patient Trust
As machine learning becomes more integrated into periodontal care, ethical concerns and patient trust take centre stage. Messina et al. (Frontiers in Dental Medicine) highlight a key challenge:
the limited interpretability of many deep learning models may hinder clinician trust and complicate accountability in clinical decision-making [1].
When AI suggests a treatment path without a clear explanation, both dentists and patients may feel uncertain about following its recommendations.
Algorithmic bias is another concern. If training datasets fail to represent diverse populations, the resulting models could deliver inequitable care [15]. This issue is particularly relevant in Australia’s multicultural society, where oral health needs and risk factors can vary widely.
The ADA stresses the importance of prioritising patient safety, quality of care, continuity of care, and data privacy and security in all AI applications [15]. Transparency is crucial – dentists must explain AI’s role in clinical decisions, ensuring patients understand that technology supports, but does not replace, professional judgement.
Lastly, the ADA warns against patients relying on generative AI tools like ChatGPT for self-diagnosis. These systems can produce content that sounds credible but may be misleading or even harmful. Dentists should educate patients on the risks of such tools and emphasise the importance of professional verification for any AI-generated health information.
Conclusion
Machine learning is transforming how periodontal disease is predicted and managed, with accuracy rates ranging from 73% to 99.4%. In many cases, these models match or even outperform specialists. For example, HC-Net+ achieved an AUROC of 94.2%, significantly higher than the 85.6% achieved by specialists [3][4]. This technology holds particular promise for regional and underserved areas, enabling general practitioners to provide care that rivals specialist expertise.
However, realising this potential comes with its own set of challenges. One major issue is the lack of consistent case definitions and high-quality imaging, which could lead to biased AI outputs [1][4]. The 2017 AAP/EFP classification offers a pathway to standardisation, but its broader adoption across Australian dental practices is crucial for achieving reliable results. This highlights the importance of developing AI models that are both explainable and trustworthy.
The complexity of many deep learning models often makes them difficult for clinicians to trust. As Mohammed Jafer et al. point out:
AI should be seen as a tool that helps doctors make better decisions and not as a way to replace their knowledge and skills [3].
Incorporating explainable AI frameworks can address this concern, allowing clinicians to better understand and validate the model’s predictions, ensuring that professional judgement remains central to patient care.
Ethical considerations also play a critical role. The Australian Dental Association emphasises that patient safety must be the primary consideration for any dental AI system [15]. This includes safeguarding data privacy, reducing algorithmic bias by using diverse training datasets, and ensuring AI tools operate under the supervision of qualified practitioners rather than independently.
To fully integrate machine learning into periodontal care, further research is needed. Longitudinal datasets, multicentre validation studies, and robust regulatory frameworks will be key to ensuring these technologies are both effective and safe. By tackling these challenges, Australian dental practices can leverage machine learning to provide more precise and accessible care for periodontal disease.
FAQs
How accurate is AI for detecting periodontal disease in real clinics?
AI has shown impressive accuracy in identifying periodontal disease within clinical settings. Research indicates that it can even surpass specialists in diagnosing stages II–IV periodontitis. Additionally, AI excels at analysing radiographs, making it a valuable tool for early detection. These advancements underscore how AI can assist dental professionals in achieving more precise diagnoses and improving patient care.
What data does an AI model need to assess gum disease risk?
AI models designed to evaluate the risk of gum disease rely on a mix of data sources. These include dental radiographs like panoramic or periapical X-rays, which help spot bone loss and signs of tissue inflammation. They also use clinical measurements, such as probing depths and bleeding on probing, alongside lifestyle factors like smoking habits and oral hygiene routines. This combination allows the models to detect early warning signs, assess severity, and predict how the condition might progress, paving the way for more tailored and prompt care.
Who is responsible if an AI tool gets a diagnosis wrong in Australia?
In Australia, healthcare professionals bear the responsibility for diagnoses made with the help of AI tools. While these tools can assist, clinicians must rely on their professional judgment to ensure AI is applied appropriately in their practice. Importantly, AI does not absolve practitioners of accountability – clinicians remain fully responsible for verifying diagnoses and making informed treatment decisions. If AI is used unsafely or unethically, practitioners may face liability for adverse outcomes, in line with Australian regulations and professional standards.
Related Blog Posts
- AI Research in Oral Disease Detection: Key Findings
- AI in Dentistry: Predicting Periodontal Disease
- How AI Predicts Periodontal Bone Loss
- AI vs Traditional Periodontal Diagnosis
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





