







How Indirect Bonding Improves Bracket Placement Accuracy

Indirect bonding (IDB) makes placing orthodontic brackets more precise and efficient than direct bonding (DBB). By first positioning brackets on a model outside the mouth, orthodontists avoid common challenges like saliva and limited visibility. This method reduces errors in placement, shortens treatment time, and delivers better outcomes. Key benefits include:
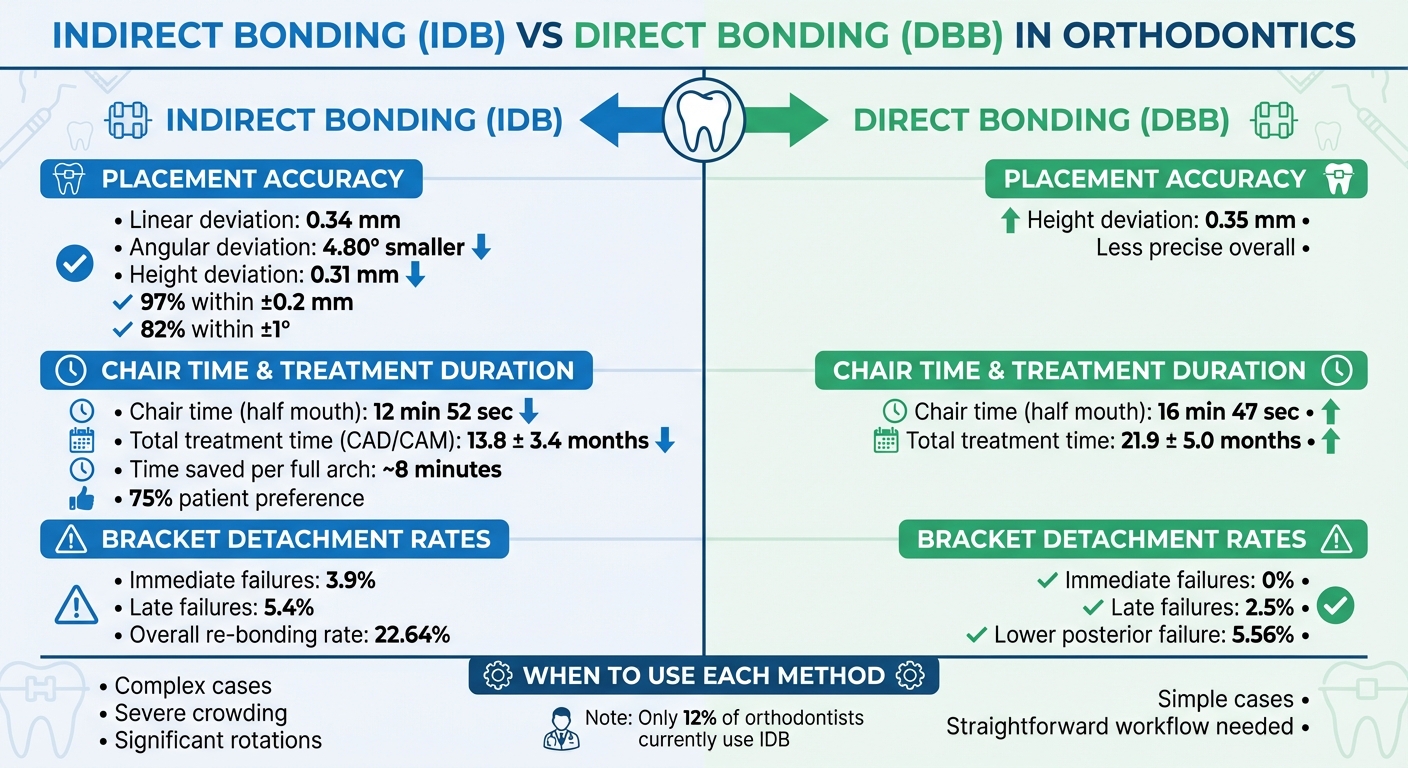
- Higher accuracy: Studies show IDB reduces linear deviations to 0.34 mm and angular deviations by 4.80° compared to DBB.
- Shorter chair time: Bonding half a mouth takes ~12 minutes with IDB versus ~16 minutes with DBB.
- Faster treatment progress: CAD/CAM IDB reduces treatment time to 13.8 months on average, compared to 21.9 months with DBB.
However, IDB requires more lab preparation and has higher bracket detachment rates (3.9% immediate failures vs 0% for DBB). It’s ideal for complex cases, but simpler cases may benefit from DBB due to its straightforward process. Choosing the right method depends on the case complexity, available tools, and patient preferences.
Indirect vs Direct Bonding: Accuracy, Time, and Treatment Comparison
Indirect Bonding Tips live demo for braces – by Dr Vandana Katyal, Sydney Orthodontist
Benefits of Indirect Bonding Compared to Direct Bonding
Indirect bonding, which involves placing brackets in a controlled lab setting rather than directly in the mouth, offers several clear advantages. These benefits stem from its ability to enhance precision, save time, and streamline treatment.
Improved Bracket Placement Accuracy
One of the standout benefits of indirect bonding is its precision. By working on dental models in a lab, practitioners gain a clear, unobstructed view and the opportunity to fine-tune bracket placement. This method often incorporates CBCT (cone-beam computed tomography) data, which aligns brackets with root positions rather than just the visible crown [3].
A 2024 split-mouth study highlighted this accuracy, showing that indirect bonding resulted in 0.34 mm smaller deviations in translation and 4.80° smaller deviations in orientation compared to direct bonding [1]. Furthermore, when measuring bracket height, indirect bonding showed an average deviation of 0.31 mm, slightly outperforming direct bonding’s 0.35 mm [2]. Professor Lincoln Issamu Nojima from Universidade Federal do Rio de Janeiro summed it up perfectly:
errors associated with bracket positioning were minimised when indirect bonding was chosen over direct bonding, under any of three aspects of observation: height, mesiodistal position and angulation
[4]. These precise placements lead to smoother clinical workflows and fewer adjustments later.
Reduced Chair Time
Indirect bonding also significantly cuts down on chair time. Using a pre-loaded transfer tray, all brackets can be bonded at once, avoiding common challenges like saliva interference and limited visibility. Research has shown that computer-aided indirect bonding takes just 12 minutes and 52 seconds to bond half a mouth, compared to 16 minutes and 47 seconds for direct bonding [10]. For a full arch, this method can save approximately 8 minutes per patient. Additionally, about 75% of patients in one study favoured indirect bonding for its shorter appointments [1]. Less time spent in the chair also supports faster overall treatment by reducing the need for repositioning brackets.
Quicker Treatment Progress
The heightened accuracy of indirect bonding translates into faster treatment progress. Brackets placed with precision allow archwires to apply optimal forces, minimising the need for ongoing adjustments. A study comparing bonding methods found that CAD/CAM-customised indirect bonding reduced total treatment time to 13.8 ± 3.4 months. In contrast, direct bonding required 21.9 ± 5.0 months, and traditional indirect bonding methods averaged 16.9 ± 4.1 months [2]. This reduction in treatment time is largely due to fewer corrections needed for bracket misplacement.
Research Findings on Indirect Bonding
Appointment Time and Treatment Length Studies
Studies consistently highlight that indirect bonding can significantly cut down the time patients spend in the chair. For instance, computer-aided indirect bonding reduces chairside time to 12 minutes 52 seconds for half a mouth, compared to 16 minutes 47 seconds with direct bonding [10]. However, when factoring in the entire process, including digital planning and lab work, the total time extends to 28 minutes 14 seconds [10]. This still results in a time saving of about 8 minutes per patient for a full arch.
Interestingly, a systematic review of eight randomised controlled trials involving 247 participants backed these findings, confirming that indirect bonding requires less chairside time [11]. Despite the extra preparation required, most patients leaned towards indirect bonding due to its shorter appointment duration [1]. It’s worth noting, though, that the overall treatment length and number of appointments remained comparable between indirect and direct bonding methods [11]. These time savings align with the precision benefits discussed earlier.
Bracket Failure Rates and Placement Precision
Beyond saving time, the precision of bracket placement plays a crucial role in treatment success. Research shows that digital workflows lead to significant improvements in bracket positioning, with deviations generally staying within acceptable clinical limits [1][6]. This enhanced accuracy translates into better treatment outcomes.
As researchers from the University of Bari "Aldo Moro" explained:
Indirect bonding is more predictable and precise than direct bonding. Indirect bonding has a greater impact on minimising bracket placement errors than direct bonding
[8].
Despite these advantages, indirect bonding isn’t without its challenges. A 2024 trial reported 3.9% immediate bonding failures for indirect bonding compared to 0% for direct bonding, as well as 5.4% late failures versus 2.5% for the direct method [1]. Additionally, a larger study involving 2,531 teeth found an overall re-bonding rate of 22.64% for indirect bonding. Of these, 15.09% were due to bonding failures and 7.55% resulted from position errors. The study also observed higher failure rates in mandibular teeth and among male patients under 20 years old [12].
sbb-itb-2be92ed
Drawbacks and Practical Considerations
While indirect bonding offers improved precision and efficiency, it comes with its own set of challenges, particularly in workflow and bracket detachment, that require careful consideration.
Laboratory Work and Technical Requirements
Indirect bonding demands significantly more preparatory work compared to direct bonding. It involves either traditional dental impressions and plaster casts or modern digital tools like intraoral scanners, CAD/CAM software, 3D printers, and specialised post-processing equipment such as ultrasonic cleaners and nitrogen-environment light-curing units. While this method reduces clinical chairside time, it increases overall patient time due to the complex preparation process [6][1]. The need for such advanced equipment and expertise has likely contributed to the fact that only about 12% of orthodontic clinicians currently use indirect bonding, despite its availability for over 50 years [6].
Another challenge lies in the time commitment. The digital planning and lab fabrication phases can be time-intensive, offsetting the time saved during clinical application [1][13]. Dr Chun-Hsi Chung from the University of Pennsylvania highlights this point:
Indirect bonding is more technique sensitive and requires more laboratory procedures and time
[2]. Many practices face difficulties in overcoming the learning curve required for both clinical application and lab processes. Inconsistent tray fabrication is a frequent issue, leading some practitioners to abandon the technique altogether [14]. These technical hurdles also increase the risk of complications during bracket removal.
Bracket Detachment Concerns
The complexities of indirect bonding extend beyond the lab, contributing to higher bracket detachment rates compared to direct bonding. Stress during tray removal, especially before the adhesive has fully cured, is a significant factor [4]. The posterior section of the lower arch is particularly susceptible, with one 15-month study reporting a bracket failure rate of 17.54% for indirect bonding, compared to just 5.56% for direct bonding in this region [9].
Several factors contribute to these elevated failure rates. Issues like poorly fitting trays caused by impression distortions, moisture contamination during full-arch tray insertion, and high lip pressure all play a role [1][4][14]. To mitigate these risks, clinicians can use adhesion boosters containing biphenyl dimethacrylate and hydroxyethyl methacrylate, which enhance resin penetration into etched enamel [7]. Additionally, opting for silicone-based trays instead of single vacuum-formed materials can improve dimensional stability and provide more accurate bracket transfers [5].
While indirect bonding has clear advantages, addressing these technical and procedural challenges is essential for its broader adoption and success.
Indirect Bonding in Current Orthodontic Practice
Digital indirect bonding offers impressive accuracy, reducing translation deviations by 0.34 mm and orientation deviations by 4.80°. Notably, 97% of linear deviations and 82% of angular deviations fall within ±0.2 mm and ±1°, respectively [1][6]. This level of precision leads to fewer mid-treatment adjustments and more predictable clinical outcomes. However, achieving this accuracy involves additional preparation steps, which can complicate the workflow.
The challenges of indirect bonding mainly revolve around the complexity of the process and bracket retention issues. This method demands extra time for digital planning and laboratory work. Studies show that bonding failure rates are higher with indirect bonding – 3.9% immediately and 5.4% later – compared to 0% and 2.5% for direct bonding [1]. As researcher A. Patano points out:
Indirect bonding is more predictable and precise than direct bonding
[8]. These considerations highlight the trade-off between precision and procedural efficiency, influencing how clinicians choose their bonding approach.
The decision to use indirect bonding often depends on the complexity of the case. For patients with severe crowding or significant rotations, indirect bonding is particularly effective [7]. On the other hand, for simpler cases, the straightforward workflow and lower failure rates of direct bonding may be the better option. Factors like the availability of CBCT imaging for improved root visualisation and the patient’s willingness to cooperate with longer appointments also play a role in determining the best method [3]. By weighing these factors, orthodontists can optimise treatment efficiency and outcomes.
Advancements in digital workflows, such as intraoral scanning and 3D printing, are making indirect bonding more accessible. Despite these technological improvements, the core principle remains unchanged: accurate bracket placement is essential for successful treatment. By mastering both direct and indirect bonding techniques, orthodontists can customise their approach, ensuring the right balance of precision, efficiency, and reliability for each patient.
FAQs
What are the benefits of using indirect bonding for orthodontic brackets?
Indirect bonding brings a range of benefits compared to direct bonding. One of its standout advantages is the improved accuracy and precision it offers in placing brackets. This level of precision plays a key role in achieving the best possible orthodontic outcomes.
Another major perk? It cuts down chair-side time. With fewer steps to handle during the appointment, the process becomes smoother and more efficient for both the patient and the orthodontist.
What’s more, indirect bonding allows for pre-planning using a model, which is especially helpful for handling more complex cases. This approach not only boosts consistency and control but also reduces the chances of errors during bracket placement, ensuring a more streamlined and effective treatment process.
How does indirect bonding improve treatment efficiency?
Indirect bonding improves the efficiency of orthodontic treatment by ensuring brackets are placed with precision. This reduces the likelihood of errors and minimises the need for frequent adjustments during follow-up appointments. The method allows multiple brackets to be positioned correctly in a single session, saving time for both patients and orthodontists.
By simplifying the process, indirect bonding helps cut down on chair time and reduces the total number of visits, making the treatment experience quicker and more convenient.
What are the challenges of using indirect bonding for orthodontic brackets?
Indirect bonding is known for its precision in bracket placement, but it does come with a few hurdles. The process demands a high level of skill and attention to detail, as every step – from taking accurate impressions to setting up the model and fabricating the transfer tray – needs to be spot on. Mistakes at any stage can ripple through and impact the final outcome. Even when using advanced digital workflows, small inaccuracies can creep in, particularly during 3D printing.
Another consideration is the cost. Indirect bonding tends to be more expensive due to the materials and lab work involved in creating the transfer trays. If the tray doesn’t fit properly upon seating, a second bonding attempt might be necessary. This not only increases chair-side time but can also affect the patient’s overall experience. Unlike direct bonding, where adjustments can be made on the fly, indirect bonding offers less flexibility. Repositioning brackets often means starting the process over from scratch.
While this method does provide greater precision, it requires careful planning and a skilled approach to minimise potential issues.
Related Blog Posts
- Orthodontic Force Measurement: Why Accuracy Matters
- Ceramic Bracket Bonding: Adhesive Types Compared
- Digital Orthodontics: CAD/CAM Workflow Explained
- Ultimate Guide to Digital Orthodontic Systems
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





