







Cementum: Microscopic Anatomy Explained

Cementum is the mineralised tissue covering the roots of your teeth, anchoring them to the jawbone through the periodontal ligament. Unlike other dental tissues, it lacks blood vessels and nerves but continues to grow throughout life, compensating for wear. Its resistance to resorption makes it crucial during orthodontic treatments, while its ability to repair itself helps maintain oral health.
Key points about cementum:
- Primary Function: Anchors teeth via Sharpey’s fibres.
- Types: Four types – Acellular Extrinsic (AEFC), Cellular Intrinsic (CIFC), Cellular Mixed (CMSC), and Acellular Afibrillar (AAC) – each with unique roles and locations.
- Composition: 50–60% inorganic hydroxyapatite and 90% Type I collagen in the organic matrix.
- Self-Repair: Can mend damage to roots, such as fractures or resorption.
- Ageing: Thickness can triple between ages 20 and 60.
Cementum plays a protective role by sealing dentine and supporting periodontal health. However, gum recession or periodontal disease can compromise it, leading to sensitivity, caries, or bacterial infiltration. Dental care, including scaling and root planing, must balance removing damaged cementum while preserving healthy layers for ligament reattachment.
Understanding cementum’s structure and function is essential for maintaining tooth stability and oral health. Regular dental check-ups help detect and address issues early, ensuring long-term protection of this vital tissue.
Cementum: Structure, Types and Functions
4 Types of Cementum
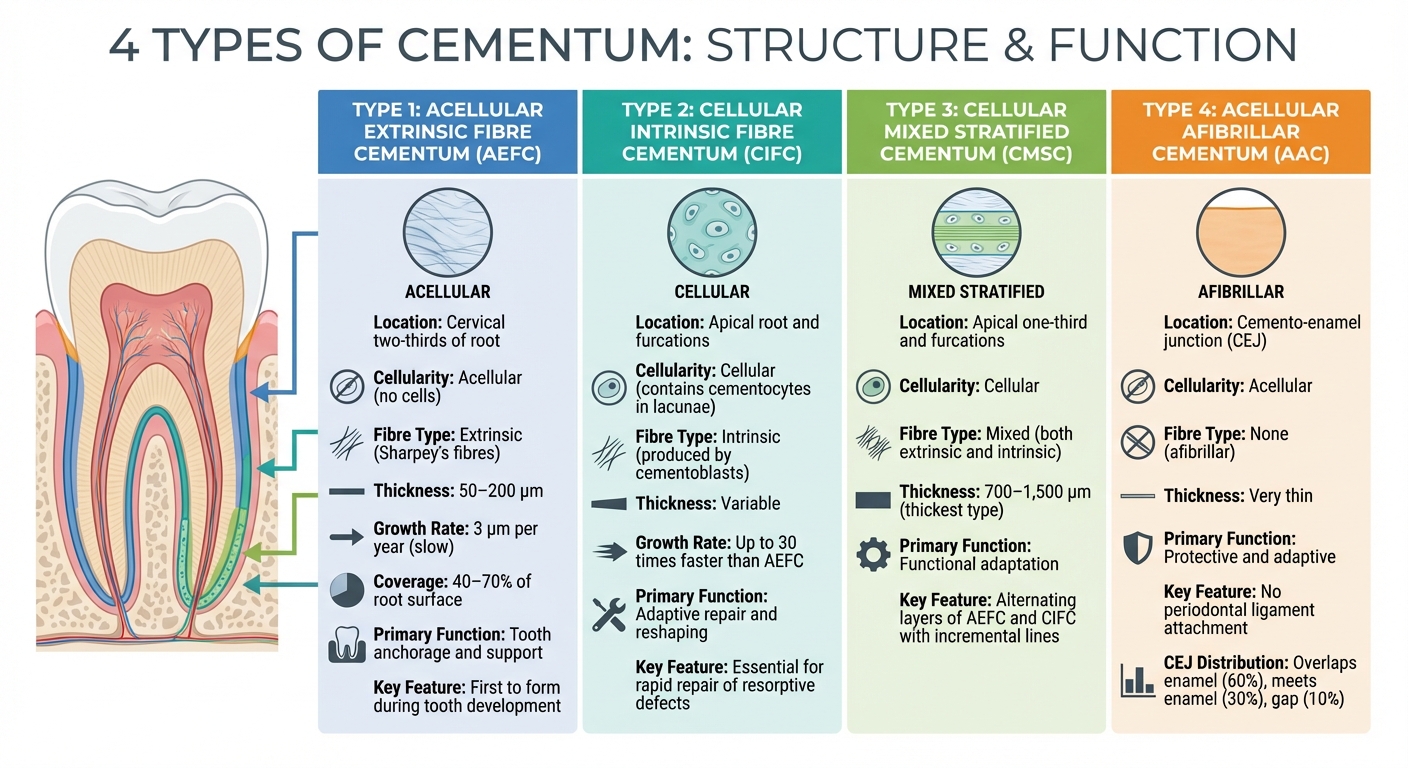
Four Types of Cementum: Location, Structure and Function Comparison
Cementum, the mineralised tissue covering the tooth root, comes in four distinct types. These variations are tied to their structure, location, and specific roles. The classification hinges on two factors: whether the cementum contains cells (cellular or acellular) and the type of collagen fibres present (extrinsic, intrinsic, or none). Interestingly, approximately 90% of the organic matrix in human cementum is made up of Type I collagen [4]. The distribution of these types reflects the tooth’s developmental journey and its functional needs. Below is a breakdown of each type’s characteristics and role.
| Cementum Type | Primary Location | Cellularity | Fibre Type | Thickness | Primary Function |
|---|---|---|---|---|---|
| Acellular Extrinsic (AEFC) | Cervical two-thirds of root | Acellular | Extrinsic (Sharpey’s) | 50–200 μm | Tooth anchorage/support |
| Cellular Intrinsic (CIFC) | Apical root, furcations | Cellular (cementocytes) | Intrinsic | Variable | Adaptive repair/reshaping |
| Cellular Mixed (CMSC) | Apical one-third, furcations | Cellular | Mixed (both types) | 700–1,500 μm | Functional adaptation |
| Acellular Afibrillar (AAC) | Cemento-enamel junction | Acellular | None (afibrillar) | Very thin | Protective/adaptive |
Acellular Extrinsic Fibre Cementum (AEFC)
AEFC is the first cementum type to form during tooth development. Found in the cervical and middle portions of the root, it is packed with Sharpey’s fibres, which run perpendicular to the root surface. These fibres provide a robust anchor for the periodontal ligament. AEFC ranges in thickness from 50 to 200 μm and typically covers 40% to 70% of the root surface [4]. Since it lacks cells, it forms slowly – about 3 μm per year [8]. However, its thin layer is vulnerable, especially during procedures like aggressive root planing, which can strip away this protective layer and expose the dentine beneath.
Cellular Intrinsic Fibre Cementum (CIFC)
CIFC is found in the apical regions and furcation areas of multi-rooted teeth. This type contains cementocytes housed in lacunae, and its collagen fibres are intrinsic, produced by cementoblasts rather than periodontal ligament fibroblasts. CIFC forms much faster than AEFC – up to 30 times quicker [8] – making it essential for repair. As Patricia Furtado Gonçalves from UNICAMP‘s School of Dentistry notes:
"Only cellular intrinsic fibre cementum can repair a resorptive defect of the root in a reasonable time, due to its capacity to grow much faster than any other type of cementum" [5].
Cellular Mixed Stratified Cementum (CMSC)
CMSC is located in the apical third of the root and furcation areas. It is notably thicker than other types, ranging from 700 to 1,500 μm [4]. This cementum type alternates layers of AEFC and CIFC, creating a stratified look with incremental lines. Tsuneyuki Yamamoto from Hokkaido University Graduate School of Dental Medicine explains:
"CMSC distribution and thickness of a particular tooth may reflect its past history of eruption rather than masticatory function" [4].
Acellular Afibrillar Cementum (AAC)
AAC is found in isolated patches near the cemento-enamel junction (CEJ) and sometimes extends onto the enamel surface. It has neither cells nor collagen fibres, which means it doesn’t anchor periodontal ligament fibres. Instead, its role is purely protective or adaptive. At the CEJ, the cementum-enamel relationship follows the "OMG" rule: cementum overlaps enamel in 60% of cases, meets enamel in 30%, and leaves a gap in 10% [7].
Microscopic Structure of Cementum
Mineral and Organic Components
Cementum consists of 50% to 60% inorganic hydroxyapatite crystals [Ca10(PO4)6(OH)2] and an organic matrix dominated by Type I collagen, which makes up about 90% of its fibres. Non-collagenous proteins, such as bone sialoprotein and osteopontin, play a role in regulating mineralisation and helping cells attach to the tissue [2][5][6]. The hydroxyapatite crystals themselves are relatively small, measuring between 1–4 μm in length [6], and are less mineralised compared to those in dentine or enamel. Type III collagen contributes roughly 5% to the overall collagen content [2][5][6]. As Michel Goldberg explains:
"Type I collagen accounts for 90% of all collagens that develops into intrafibrillar apatite crystals" [2].
What makes cementum distinct from bone at the molecular level are its specific proteins, such as Cementum Attachment Protein (CAP) and Cementum Protein-1 (CEMP1) [2][5]. Additionally, cementum contains trace minerals like magnesium (0.5%–0.9%), fluoride (up to 0.9% of ash weight – higher than in other dental tissues), and sulphur (0.1%–0.3%) [5]. These components collectively ensure that cementum can effectively anchor teeth in place.
Cementocytes and Canaliculi
Cementum’s cellular structure further defines its functionality. In certain types of cementum, known as cellular cementum, cementoblasts become embedded in the mineralising matrix and transform into cementocytes. These cementocytes are housed in small cavities called lacunae, while their cytoplasmic extensions spread through narrow channels called canaliculi. These canaliculi are oriented toward the periodontal ligament, allowing cementocytes to access nutrients through diffusion [5][7]. This system ensures the tissue remains viable and can adapt to changing functional demands.
Incremental Lines in Cementum
Another notable feature of cementum is the presence of incremental lines, which reveal its deposition history. These lines, also called Salter lines or resting lines, appear as dark bands under a microscope and represent periods of cementum deposition. They are more mineralised than the surrounding matrix [2][4][5]. In acellular extrinsic fibre cementum (AEFC), these lines indicate resting phases during intermittent deposition. Tsuneyuki Yamamoto from Hokkaido University highlights:
"The incremental lines are highly mineralised and are thus regarded as resting lines, formed in resting phases during intermittent AEFC formation" [10].
In cellular mixed stratified cementum (CMSC), these lines divide the tissue into distinct layers. The varying widths between these lines reflect fluctuations in cementum deposition rates over time [6]. These patterns not only document the tooth’s developmental history but also serve as a valuable tool for age estimation in dental histology, showcasing cementum’s ability to adapt dynamically to functional pressures.
sbb-itb-2be92ed
How Cementum Develops
Understanding how cementum forms sheds light on its role in providing anchorage and maintaining periodontal health.
Cementogenesis and Hertwig’s Epithelial Root Sheath
The process of cementum formation, or cementogenesis, begins when Hertwig’s Epithelial Root Sheath (HERS) starts to break down. As HERS grows toward the root apex, it stimulates cells in the dental papilla to transform into odontoblasts, which then form root dentine. When HERS disintegrates, mesenchymal cells from the surrounding dental follicle come into contact with the newly formed dentine. This interaction prompts these mesenchymal cells to differentiate into cementoblasts, the cells responsible for creating cementum.
Before HERS fully disintegrates, it may deposit a thin layer of intermediate cementum, about 10 μm thick, to seal the dentinal tubules. Even after breaking down, remnants of HERS remain as epithelial cell rests of Malassez. Cementoblasts then produce an organic matrix, known as precementum or cementoid, which is rich in collagen fibrils. This matrix later undergoes mineralisation, transforming into the mature, layered cementum.
Mineralisation and Lamellae Formation
Once the collagen-based precementum is laid down, mineralisation solidifies it into cementum. This transformation occurs through the deposition of hydroxyapatite crystals, which initially form between collagen fibres and later within them. Non-collagenous proteins like bone sialoprotein and osteopontin play a key role in regulating this process [4]. The balance between inorganic pyrophosphate (PPi), which inhibits mineralisation, and tissue non-specific alkaline phosphatase (TNAP), which promotes it by breaking down PPi, is critical for controlling how quickly minerals are deposited [2].
Cementum forms in layers rather than continuously, with incremental lines marking periods of rest in its deposition [9]. In cellular intrinsic fibre cementum (CIFC), the collagen fibrils are arranged in a unique "twisted plywood" pattern. Each layer has collagen fibrils aligned in one direction, with the orientation rotating in the next layer. This creates alternating lamellae about 2.5 μm thick [4]. This structure enhances cementum’s ability to withstand stresses from multiple directions. As Tsuneyuki Yamamoto explains:
"all collagen fibrils run parallel in a given plane, and their direction rotates from plane to plane" [4].
These developmental processes are key to cementum’s durability and its importance in maintaining periodontal health.
Clinical Applications of Cementum Knowledge
Cementum’s microscopic structure plays a crucial role in periodontal treatments and long-term oral health maintenance.
Cementum’s Role in Periodontal Health
Cementum is more than just a tooth anchor; it’s essential for periodontal stability. It provides the attachment site for Sharpey’s fibres of the periodontal ligament, which secure teeth to the alveolar bone. Additionally, cementum seals dentinal tubules, protecting the underlying dentine and reducing both sensitivity and infection risks [1][5][7].
However, periodontal disease can compromise cementum. Its permeability increases, allowing bacterial byproducts to infiltrate. Studies reveal that bacterial lipopolysaccharides can penetrate up to 70 μm into diseased cementum [1][6]. As Pocket Dentistry highlights [6]:
"Infected cementum has been characterised as a reservoir of periodontopathogenic bacteria."
This bacterial infiltration complicates treatment, requiring practitioners to carefully remove infected tissue while preserving enough healthy cementum to enable periodontal ligament reattachment. These challenges underscore the importance of precise root surface management.
Root Surface Treatment Considerations
Cementum’s protective role makes its preservation a priority during periodontal therapy. Procedures like scaling and root planing must strike a balance between removing contaminated cementum and retaining the acellular extrinsic fibre cementum (AEFC), which is critical for ligament attachment [11][6]. Bacterial toxins are often found within the top 10 to 12 μm of the cementum, but in some cases, they can penetrate deeper [6].
The cervical third of the root is particularly vulnerable during instrumentation, as the AEFC here is only about 50 μm thick [6]. Over-instrumentation in this area can expose dentinal tubules, leading to hypersensitivity and a higher risk of root caries [7]. On the other hand, insufficient debridement may leave behind bacterial deposits, hindering healing.
To address these challenges, modern regenerative techniques use biomaterials like Enamel Matrix Derivative and Fibroblast Growth Factor 2 to encourage new cementum growth and improve ligament reattachment [11][2].
Professional Assessment of Cementum Health
Routine professional evaluations are essential for monitoring cementum health and identifying early signs of periodontal issues. A detailed understanding of cementum’s microstructure is vital for these assessments. Typical evaluations include measuring periodontal probing depths, checking for gingival recession, and identifying areas of exposed or damaged cementum.
At Complete Smiles Bella Vista, periodontal evaluations are a key part of routine care. These assessments help detect changes in cementum health early, enabling timely interventions such as scaling, root treatments, or regenerative procedures.
Maintaining cementum integrity involves both professional care and patient commitment to good oral hygiene. Over time, cementum thickens, reinforcing its role in stabilising teeth and supporting oral health.
Conclusion
Key Takeaways
Cementum is the mineralised tissue covering the roots of teeth, anchoring them to the periodontal ligament. It stands out for being avascular and non-innervated, with a strong resistance to resorption – an important factor during orthodontic treatments. This guide has explored how acellular cementum provides structural support, while cellular cementum plays a role in adaptation and repair.
Cementum is composed of around 45–50% inorganic hydroxyapatite and 50–55% organic matrix, with Type I collagen making up 90% of the organic content [3][8]. Cementocytes, located in lacunae, use canaliculi to connect with the periodontal ligament for nutrient exchange. Some key features of cementum formation include:
- Incremental lines that reflect periodic deposition
- Acellular cementum forming slowly at about 3 μm per year
- Cellular cementum growing up to 30 times faster [8]
The development of cementum, or cementogenesis, is driven by Hertwig’s epithelial root sheath. This process is especially relevant in periodontal care, as bacterial lipopolysaccharides can penetrate up to 70 μm into diseased cementum [1][6]. Clinicians face the challenge of removing contaminated tissue while preserving healthy cementum to support the reattachment of the periodontal ligament.
Why Professional Dental Care Matters
The insights into cementum’s role highlight the importance of maintaining its integrity for long-term periodontal health. Since cementum lacks nerve endings, issues like root caries or resorption can develop silently, often going unnoticed until they are advanced. Research shows that microscopic cementum resorption affects around 90.5% of adult teeth, and its thickness typically triples between the ages of 20 and 60 [1].
Regular professional dental check-ups are crucial for early detection of issues like gingival recession, exposed cementum, or damaged areas. Periodontal procedures such as scaling and root planing can remove infected layers containing bacterial toxins, while regenerative treatments may help stimulate new cementum growth.
At Complete Smiles Bella Vista, periodontal evaluations are a cornerstone of routine care, helping to identify and address cementum-related changes before they lead to complications.
Understanding cementum’s unique structure and its ability to regenerate highlights the importance of timely dental care. By combining professional treatment with consistent oral hygiene, you can protect cementum integrity, ensuring better tooth stability and overall periodontal health in the long run.
FAQs
What makes cementum unique compared to other dental tissues?
Cementum is a unique, mineralised tissue that forms a protective layer over the roots of teeth. What sets it apart from other dental tissues is that it is avascular, meaning it doesn’t contain blood vessels. Its main job is to anchor the periodontal ligament, which plays a crucial role in keeping the tooth firmly attached to the jawbone.
One of its standout characteristics is its stability. Unlike bone, which goes through constant reshaping and remodelling, cementum changes very little over a lifetime. This consistency is vital for ensuring long-term tooth support and maintaining overall dental health.
How does cementum contribute to orthodontic treatments?
Cementum plays a crucial role in orthodontic treatments by serving as the attachment surface for periodontal ligament fibres. These fibres are essential for enabling controlled tooth movement while maintaining the stability of teeth throughout the treatment process.
By anchoring the periodontal ligament, cementum helps evenly distribute the forces applied during orthodontic adjustments. This ensures that tooth realignment is both effective and safe. This tiny but essential tissue supports the health and function of the structures that hold your teeth in place during orthodontic care.
What impact does periodontal disease have on cementum?
Periodontal disease can harm the cementum, the thin layer that coats the tooth root. This damage may weaken the periodontal fibres, which play a key role in supporting the tooth and keeping it stable.
Without timely treatment, this condition can jeopardise the health of the tooth and nearby tissues, increasing the risk of tooth mobility or even loss. Addressing periodontal disease early is essential to safeguard the cementum and maintain overall oral health.
Related Blog Posts
- Stem Cells in Periodontal Regeneration: Current Trials
- How Dentists Assess Crown Lengthening Candidates
- What Is Crown Lengthening?
- Biomimetic Tooth Restoration: Key Benefits
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





