







Bioceramic vs. Resin-Based Sealers: Comparison

When deciding between bioceramic and resin-based sealers for root canal treatments, the choice largely depends on the case specifics. Both sealers achieve similar clinical success rates (~96%), but they differ in their composition, handling, and long-term behaviour. Here’s a quick breakdown:
- Bioceramic Sealers: Known for their bioactivity, they chemically bond to dentine, promote healing, and work well in moist conditions. They are highly biocompatible, with minimal shrinkage and slight expansion during setting. However, they can be challenging to remove during retreatment and may cause discolouration in certain cases.
- Resin-Based Sealers: These offer excellent adhesion and are easier to remove if retreatment is needed. They require a dry canal for optimal performance and may exhibit polymerisation shrinkage and initial cytotoxicity during setting.
Quick Comparison
| Feature | Bioceramic Sealers | Resin-Based Sealers |
|---|---|---|
| Primary Components | Calcium silicates | Epoxy or salicylate resin |
| Setting Mechanism | Hydraulic (moisture needed) | Chemical polymerisation |
| Volume Change | Slight expansion or stable | Prone to shrinkage |
| Bioactivity | Promotes healing | Non-bioactive |
| Cytotoxicity | Lower | Higher (when unset) |
| Retreatment | Difficult to remove | Easier to remove |
| Best Use Cases | Moist canals, large lesions | Dry canals, retreatment |
Both sealers are effective, but choosing the right one depends on factors like canal anatomy, obturation technique, and the likelihood of retreatment. Tailor your choice to the specific needs of each case for the best outcomes.
Bioceramic vs Resin-Based Root Canal Sealers Comparison Chart
SELECTION OF ROOT CANAL SEALER; Is it time to shift to Bio-Ceramic Sealers?
sbb-itb-2be92ed
What Are Bioceramic Sealers?
Bioceramic sealers are hydraulic materials primarily made from calcium silicates, including tricalcium and dicalcium silicate. They also contain calcium phosphates and zirconium oxide, which enhances radiopacity [6][3]. These sealers harden through a hydration reaction, making them an excellent match for the moist conditions found inside root canals [6][3]. This sets them apart from resin-based sealers, which we’ll compare later.
Bioceramic sealers are bioactive, meaning they promote mineral formation at the sealer-dentine interface by creating hydroxyapatite – a mineral similar to bone [6][1]. This results in a chemical bond with the root canal walls, unlike the mechanical adhesion typical of other sealers [6][1].
"Unlike bioinert ceramics, bioactive materials… interact with the surrounding tissues to encourage the growth and regeneration of more durable mineralised tissues."
- Badawy RE and Mohamed DA [6]
In Australian dental practices, commonly used bioceramic sealers include TotalFill BC, BioRoot RCS, EndoSeal MTA, and Endosequence BC [6][7]. These products usually contain 5% to 35% tricalcium silicate, with 50% to 70% zirconium oxide for radiopacity [4][6].
Key Features of Bioceramic Sealers
A standout feature of bioceramic sealers is their hydrophilic nature, meaning they rely on moisture from dentinal tubules to set. This is in stark contrast to resin-based sealers, which require a completely dry canal [8][6]. This moisture-friendly property makes them easier to use during procedures.
As they set, bioceramic sealers maintain a high pH level, which provides antimicrobial and antibacterial benefits [1]. This alkaline environment helps eliminate residual bacteria in the canal system. Their small particle size ensures excellent flowability – often exceeding 20 mm in flow tests – allowing them to penetrate deep into dentinal tubules and accessory canals [8][1].
Another important characteristic is their dimensional stability. These sealers exhibit minimal shrinkage and may even expand slightly (often above 0.1%) during setting [8][1]. This slight expansion improves the apical seal and makes them ideal for single-cone obturation techniques. A study conducted at Alkhor Hospital, Hamad Medical Corporation in Qatar, between January 2019 and January 2022, examined 248 teeth. It found that TotalFill BC Sealer achieved a 96% success rate when used with the single-cone technique [1].
Advantages of Bioceramic Sealers
One of the most notable benefits of bioceramic sealers is their biocompatibility. They are generally less cytotoxic than resin-based sealers and are well-tolerated by periapical tissues [1][6]. If accidentally extruded beyond the apex, these sealers can promote bone repair rather than triggering inflammation.
Their performance in wet conditions is another major advantage. Research led by Takashi Komabayashi at the University of New England College of Dental Medicine revealed that tricalcium silicate sealers had the lowest relative microleakage compared to silicone and epoxy resin sealers [3]. Thanks to their small particle size and low contact angle, they can penetrate narrow canal spaces effectively, particularly in the apical third of the root [7].
"Bioceramic materials generate a chemical bond to dentine through the formation of bone apatite-like material upon their setting."
- Ginebra et al. [1]
Clinical studies show impressive success rates for bioceramic sealers: 95.7% to 100% in teeth with vital pulp and approximately 94.2% to 94.7% in cases with necrotic pulp [1]. Their ability to release bioactive substances encourages odontoblast differentiation, which supports healing [6].
What Are Resin-Based Sealers?
Resin-based sealers are primarily made from epoxy resins (such as Bisphenol A or F diglycidyl ether) and amines, which act as hardening agents. These sealers are typically supplied as a two-part system: a base paste and a catalyst paste. Before use, these components are mixed together. To enhance their functionality, they include radiopacifiers like zirconium dioxide, bismuth oxide, or calcium tungstate, making them detectable on radiographs.
The sealing ability of these materials comes from a polymerisation reaction between the epoxy resin and amines. This process transforms the material from a sticky paste into a rigid, durable matrix that effectively seals the root canal system. A well-known example is AH-Plus, regarded as the "gold standard" in resin-based sealers. It has a notably long setting time, averaging around 960 minutes, which is significantly longer than many bioceramic alternatives [9].
"AH-Plus is the most popular hydrophobic epoxy resin-based sealer that has been used as the gold standard material."
- Ju Kyung Lee et al. [9]
Unlike bioceramic sealers, resin-based sealers are hydrophobic, meaning they repel water and work best in a dry canal environment [9]. These sealers are highly dimensionally stable; for instance, AH-Plus exhibits minimal expansion – about 0.35% (±0.51) – even after 30 days in water [9]. Their solubility is also extremely low, around 0.3%, well within the ISO 6876 standard of ≤3% [3]. These characteristics make resin-based sealers distinct and provide a foundation for exploring their clinical performance and challenges.
Key Features of Resin-Based Sealers
Resin-based sealers are valued for their excellent adhesion to root dentine, which helps prevent bacterial leakage and fluid infiltration. Their chemical makeup allows for high flowability, enabling them to penetrate accessory canals, lateral canals, and small irregularities between the gutta-percha and dentinal walls. Methacrylate-based sealers (like RealSeal SE) achieve covalent bonding with dentine, while epoxy-based sealers (such as AH-Plus) adhere through polymerisation. Clinical research has shown that resin-based sealers deliver a success rate of around 96%, comparable to advanced bioceramic sealers [1]. However, they do have limitations that can influence their clinical effectiveness.
Limitations of Resin-Based Sealers
Despite their strong sealing properties, resin-based sealers come with certain drawbacks. One issue is polymerisation shrinkage, which can create small gaps at the sealer–dentine interface. Even a 1% shrinkage can allow bacteria to penetrate [10]. Their low solubility and hydrophobic nature can also pose challenges, especially in moist conditions, as these factors may weaken the bond [9]. Compared to bioceramic sealers, resin-based options like AH-Plus exhibit lower surface polarity and surface tension (approximately 45.84 mN/m versus 72.75–75.91 mN/m for bioceramics), making them less effective on moist dentine [11].
Another concern is their initial cytotoxicity. These sealers may release unreacted components during the setting process, which can irritate periapical tissues. However, this toxicity decreases significantly once the material has fully cured [9][3]. One of the biggest practical challenges is their reliance on a completely dry canal environment, which can be difficult to achieve consistently in clinical settings. This requirement remains a key limitation in their use.
Comparison of Bioceramic and Resin-Based Sealers
This section delves into the clinical performance of bioceramic and resin-based sealers, focusing on their sealing ability, biocompatibility, and other practical considerations.
Sealing Ability and Microbial Leakage
Bioceramic and resin-based sealers achieve their seal through entirely different mechanisms. Bioceramic sealers chemically bond to dentine by forming a bone-like material, hydroxyapatite, during setting. On the other hand, resin-based sealers rely on mechanical adhesion, infiltrating the microstructure of dentine for their seal effectiveness [1].
"Compared to AH Plus, tricalcium silicate sealers show the lowest relative microleakage among the sealers assessed."
- Takashi Komabayashi et al. [2]
One notable difference is dimensional stability. Bioceramic sealers remain stable, avoiding the polymerisation shrinkage commonly seen in resin-based sealers. Their high pH (often exceeding 12) also contributes to enhanced antimicrobial properties [1].
A retrospective study at Alkhor Hospital compared Adseal (resin-based) and TotalFill BC Sealer (bioceramic) over a minimum 12-month follow-up and found both sealers achieved a 96% success rate [1]. These findings highlight the importance of understanding their distinct sealing mechanisms when considering biocompatibility and postoperative results.
Biocompatibility and Postoperative Outcomes
Bioceramic sealers stand out due to their ability to promote mineralised tissue formation, reflecting their bioactive nature. They release calcium ions and maintain an alkaline environment (pH >12), which supports apical healing and provides bacteriostatic effects. In contrast, resin-based sealers tend to exhibit higher initial cytotoxicity, attributed to unreacted components released during the setting phase [1][5].
Clinical trials suggest no major differences in postoperative pain between bioceramic sealers (e.g., Endoseal MTA, TotalFill) and resin-based sealers (e.g., AH Plus) [1][13]. However, the efficiency of treatment varies: obturation times for molars were shorter with bioceramic sealers (198 seconds using a single-cone technique) compared to resin-based sealers (265 seconds using the continuous wave technique) [13].
When it comes to bond strength, resin-based sealers like AH Plus exhibit higher values (3.26 ± 1.06 MPa) compared to bioceramic sealers such as EndoSequence (2.38 ± 0.75 MPa). However, bioceramic sealers compensate with deeper penetration into dentinal tubules, with EndoSequence achieving a 50.34% penetration rate compared to AH Plus Jet’s 7.31% [14]. This greater penetration may offset the lower bond strength by enhancing the seal’s durability.
Comparison Table
Here’s a quick overview to help in clinical decision-making:
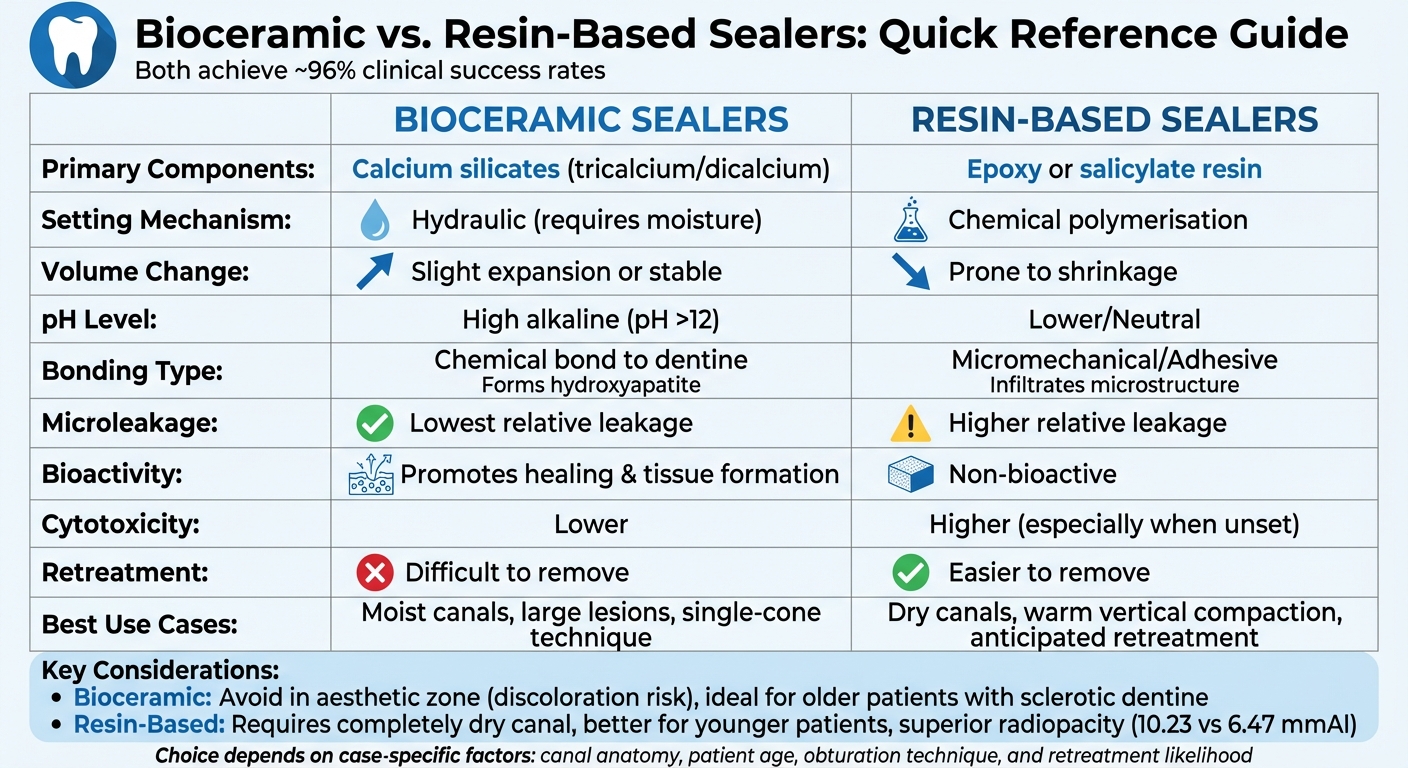
| Feature | Bioceramic Sealers | Resin-Based Sealers |
|---|---|---|
| Primary Components | Tricalcium/Dicalcium Silicates | Epoxy or Salicylate Resin |
| Setting Mechanism | Hydraulic (requires moisture) | Chemical polymerisation |
| Volume Change | Slight expansion or stable | Prone to shrinkage |
| pH Level | High (Alkaline, pH >12) | Lower/Neutral |
| Bonding Type | Chemical bond to dentine | Micromechanical/Adhesive |
| Microleakage | Lowest relative leakage [2] | Higher relative leakage |
| Bioactivity | Promotes hydroxyapatite formation | Non-bioactive |
| Cytotoxicity | Lower cytotoxicity | Higher (especially when unset) |
| Clinical Success Rate | ~96% | ~96% |
| Retreatment | Difficult to remove | Easier to remove |
This table summarises their differences, making it easier to weigh the strengths and limitations of each sealer in clinical practice.
Clinical Considerations for Dentists
When it comes to choosing the right sealer, dentists need to consider factors like canal anatomy, the obturation technique being used, and the possibility of future retreatment. Tailoring the sealer choice to the specific case helps ensure more predictable and successful outcomes.
"The choice between BC and RB sealers should be guided by case-specific factors, including anatomical considerations, patient’s dental health status, obturation techniques and clinician’s skills."
- Nature [1]
Another key aspect is the patient’s age. For older patients with sclerotic dentine, bioceramic sealers are often a better choice due to their ability to form hydroxyapatite and chemically bond to the dentine. On the other hand, younger patients with less sclerotic dentine may benefit more from resin-based sealers, which excel in micromechanical adhesion [15]. These patient-specific considerations play a significant role in determining the sealer that best suits the treatment plan.
When to Use Bioceramic Sealers
Bioceramic sealers shine in single-appointment treatments that employ the single-cone technique. Their hydraulic setting process, which relies on moisture, makes them ideal for canals that are difficult to dry. To ensure proper hydration and setting, clinicians should remove the smear layer during the final irrigation step [4].
These sealers are particularly effective for cases involving large periapical lesions. Thanks to their bioactivity, they release calcium ions and maintain a high alkalinity (pH above 8.5), which aids in faster bone healing and provides bacteriostatic effects during the setting process [5]. Clinical trials have shown that bioceramic sealers like Endoseal MTA can significantly reduce obturation time – for example, molar treatments took 198 seconds compared to 265 seconds with resin-based alternatives [16].
However, there are limitations. Avoid using bioceramic sealers in the aesthetic zone if they contain bismuth oxide, as it can lead to tooth discolouration when interacting with sodium hypochlorite or collagen [4]. Additionally, these sealers are harder to remove during retreatment, which may complicate future procedures [1].
When to Use Resin-Based Sealers
Resin-based sealers have their strengths, particularly when using the warm vertical compaction technique, which is considered the gold standard. Unlike standard bioceramic sealers, which may thicken or undergo chemical changes under heat, certain "HiFlow" versions (like EndoSequence BC HiFlow) are specifically designed to handle high temperatures [12].
These sealers are also a better choice when retreatment is anticipated, especially in cases with uncertain prognoses or complex canal anatomy that might require revision down the line [15].
Another advantage is their low solubility. For instance, AH Plus demonstrated nearly 0% solubility in distilled water, whereas TotalFill BC showed a solubility rate of 7.63% [8]. This makes resin-based sealers a reliable option in situations where long-term material stability is crucial. However, because they are hydrophobic, a dry canal environment is essential for achieving optimal adhesion, so moisture control during obturation is critical [4].
Conclusion
Bioceramic and resin-based sealers both play a crucial role in modern endodontics. Studies demonstrate that when applied correctly, they deliver similar clinical success rates. For instance, a retrospective analysis of 248 endodontically treated teeth reported an impressive 96% success rate for both types of sealers [1]. This highlights the importance of tailoring the choice of sealer to the specific needs of each case.
The main distinction between the two lies in their core characteristics. Bioceramic sealers stand out for their bioactivity and compatibility with biological tissues. They encourage hydroxyapatite formation, support tissue healing, and maintain a high level of alkalinity, which contributes to their antimicrobial properties. On the other hand, resin-based sealers, such as AH Plus, are renowned for their outstanding physical attributes. They offer superior radiopacity (10.23 mmAl compared to 6.47 mmAl for TotalFill BC) and excellent bond strength to dentine [8]. However, resin-based sealers are susceptible to polymerisation shrinkage and lack the bioactive advantages that bioceramic sealers provide. These differences underscore the trade-offs between bioactive benefits and physical performance, which are key considerations for clinicians.
FAQs
Which sealer is best if the canal can’t be fully dried?
Bioceramic sealers are often the go-to choice when the canal isn’t completely dry. These sealers offer strong sealing properties and help reduce microbial leakage, making them a more reliable option in these situations compared to resin-based sealers.
Will a bioceramic sealer make my tooth look darker?
Bioceramic sealers tend to have a lower chance of causing noticeable tooth discolouration compared to resin-based sealers, which are often linked to staining. Although slight discolouration might still occur, bioceramic sealers are generally less likely to darken the tooth’s appearance.
If I need retreatment later, which sealer is easier to remove?
Bioceramic sealers are often more challenging to remove during retreatment compared to resin-based sealers. That said, research presents varied findings, suggesting that outcomes can differ. Fortunately, there are additional techniques available to aid in their removal. Ultimately, the choice of sealer often hinges on the specific clinical requirements and the potential for retreatment in the future.
Related Blog Posts
- Nanocomposites for Pulp Regeneration: Key Features
- Ceramic Bracket Bonding: Adhesive Types Compared
- 3D Bioprinting Materials for Endodontic Repair
- Ceramic vs. Resin: Toughness in CAD/CAM Restorations
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





