







Ultrasonic Activation for Biofilm Removal: Research Insights

Ultrasonic activation, or Passive Ultrasonic Irrigation (PUI), is an effective method for removing biofilms from root canals, outperforming traditional syringe irrigation. Here’s what you need to know:
- Biofilms, especially those formed by Enterococcus faecalis, are tough to eliminate due to their dense structure and the complex anatomy of root canals.
- PUI uses high-frequency vibrations (20,000+ Hz) to create acoustic streaming and cavitation, which physically disrupt biofilms.
- Studies show PUI achieves up to 99.40% biofilm removal when the ultrasonic tip is positioned 2 mm from the apex, compared to 84.25% for syringe irrigation.
- However, its efficacy decreases in curved canals or when the tip is further from the apex. Additionally, current research lacks standardisation, making clinical application less predictable.
- Alternatives like multisonic systems (e.g., GentleWave) and laser-activated irrigation offer comparable or better results in certain cases but require specialised equipment.
Key takeaway: PUI is a reliable adjunct to root canal therapy but works best when combined with sodium hypochlorite, dynamic tip movement, and precise placement near the apex. While promising, it’s not a standalone solution and has limitations in complex cases.
VDW Dental · How To: VDW.ULTRA – Ultrasonic irrigation using IRRI S
Research Findings on Biofilm Removal with Ultrasonic Activation
Biofilm Removal Efficacy Comparison: Ultrasonic vs Manual vs Sonic Irrigation Methods
Study Models and Experimental Designs
Researchers have explored a variety of in vitro models to study biofilm removal, including extracted human teeth, bovine dentin, hydroxyapatite discs, and 3D-printed PDMS chips. These models help visualise how irrigants flow and disrupt biofilms, offering insights that are tough to replicate in actual clinical settings [6].
Most studies focus on single-species biofilms, often using Enterococcus faecalis. Others examine dual-species biofilms, such as E. faecalis paired with Streptococcus oralis, or multispecies biofilms derived from subgingival plaque [1]. The age of the biofilms varies widely, from just one day to as long as 50 days, with an average maturity of 14–18 days [1]. Mature biofilms, particularly those aged 5–6 weeks, develop honeycomb-like structures that are highly resistant to disruption [1][3].
These different models provide a foundation for evaluating how well ultrasonic activation works in removing biofilms.
How Effective is Ultrasonic Activation?
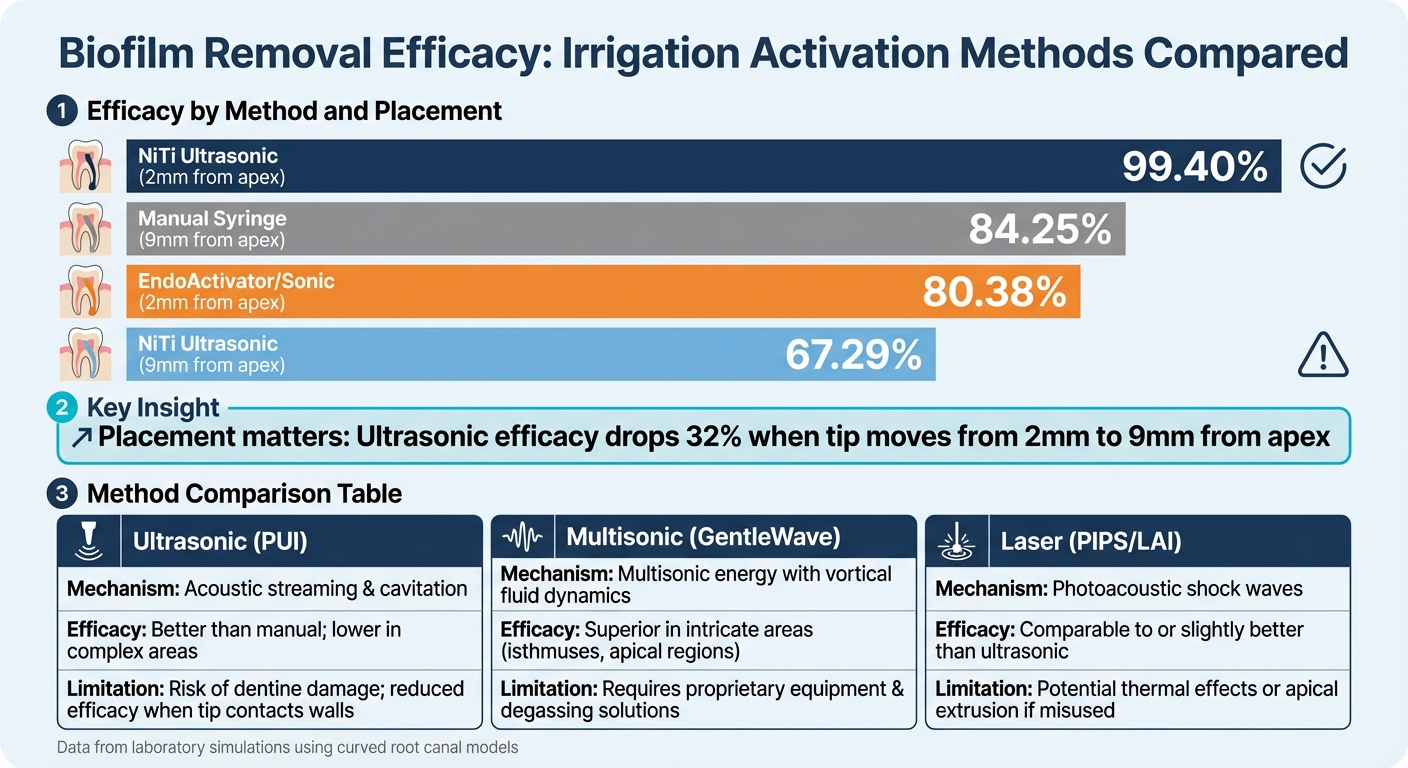
When tested in these experimental settings, ultrasonic activation consistently delivers better results than traditional irrigation methods. For instance, in simulated curved canals, NiTi ultrasonic instruments placed 2 millimetres from the apex achieved a biofilm removal rate of 99.40%. In comparison, manual syringe irrigation and sonic activation (using EndoActivator) achieved 84.25% and 80.38% efficacy, respectively [6]. However, the effectiveness of ultrasonic activation dropped to 67.29% when the ultrasonic tip was positioned 9 millimetres from the apex [6].
| Activation Method | Placement Depth | Biofilm Removal Efficacy (%) |
|---|---|---|
| NiTi Ultrasonic | 2 mm from apex | 99.40% |
| Manual Syringe | 9 mm from apex | 84.25% |
| EndoActivator (Sonic) | 2 mm from apex | 80.38% |
| NiTi Ultrasonic | 9 mm from apex | 67.29% |
Data derived from laboratory simulations using curved root canal models [6].
The highest cleaning efficiency occurs at the ultrasonic file’s anti-nodes, with a noticeable drop-off in performance just 0.5 millimetres beyond the tip [2]. While these lab results are promising, conventional methods still leave residual bacteria in over 80% of cases, particularly in the apical region and complex areas like isthmuses [3].
Limitations of Current Research
Despite encouraging laboratory outcomes, several limitations in current research need to be addressed. One major issue is the lack of standardisation in experimental protocols. Variations in factors such as power settings, ultrasonic tip sizes, irrigant concentrations, and activation durations make it difficult to directly compare results across studies [1]. As Josic et al. [1] pointed out:
Due to heterogeneity in methods among the reviewed studies, it is difficult to compare sonic-, ultrasonic- and Er:Yag laser-assisted techniques among each other and give recommendations for the most efficient method.
Another challenge is the reliance on simplified or immature biofilm models, which don’t fully capture the complexity of persistent endodontic infections. These simplified setups often overlook key anatomical features, such as severe curvatures, lateral canals, and isthmuses [6]. Furthermore, while laboratory studies often show high efficacy, clinical trials have not always confirmed that ultrasonic activation leads to better periapical healing compared to conventional syringe irrigation [5]. For example, in a dual-species biofilm study, ultrasonic activation significantly reduced bacteria, but strong regrowth was observed in all groups within five days [5].
Comparison with Other Irrigant Activation Methods
Multisonic Systems vs Ultrasonic Activation
Multisonic systems, like GentleWave, utilise a combination of multiple sound frequencies, vortical fluid dynamics, and degassing microbubbles to clean root canals effectively [3]. Unlike ultrasonic activation, the GentleWave handpiece stays in the pulp chamber rather than entering the canal itself.
Studies highlight that GentleWave achieves significantly better biofilm removal in intricate root anatomies, such as the mesial roots of mandibular molars and mesiobuccal roots of maxillary molars (p = 0.001), while also allowing for more conservative instrumentation [3]. For example, multisonic systems can effectively disinfect with minimal instrumentation (e.g. size #15/.04), whereas ultrasonic activation often requires larger instrumentation (e.g. size #35/.04) to enable the ultrasonic tip to reach the apical region [3]. However, the need for proprietary equipment and degassing solutions may make multisonic systems less accessible for some dental practices.
Next, let’s explore how laser-based methods compare to these approaches.
Laser-Activated Irrigation vs Ultrasonic Activation
Laser-activated irrigation, including Photon-Induced Photoacoustic Streaming (PIPS) with Er:YAG lasers, works through a different mechanism. These lasers generate shock waves by rapidly evaporating water, creating photoacoustic and photomechanical effects [1]. Like multisonic systems, the laser tip is generally positioned in the pulp chamber rather than within the canal.
A study comparing Er,Cr:YSGG lasers and ultrasonic activation found both methods significantly reduced bacterial loads, with no major difference in their overall effectiveness [4]. Both approaches outperformed traditional syringe irrigation, though neither was able to completely eliminate biofilm [1]. The primary challenges with laser systems are their reliance on specialised equipment and the potential risks of apical extrusion or thermal damage if not handled properly [4].
Strengths and Limitations of Each Method
Here’s a summary of the advantages and challenges associated with each technique:
| Method | Mechanism | Biofilm Removal Efficacy | Key Limitations |
|---|---|---|---|
| Ultrasonic (PUI) | Acoustic streaming and cavitation [5] | Better than manual; lower in complex areas compared to multisonic [3] | Risk of dentine damage when energy dissipates on canal walls [5] |
| Multisonic (GentleWave) | Multisonic energy with vortical fluid dynamics and degassing microbubbles [3] | Superior in intricate areas, such as isthmuses and apical regions [3] | Requires proprietary equipment and degassing solutions [3] |
| Laser (PIPS/LAI) | Photoacoustic shock waves and photomechanical streaming [1] | Comparable to or slightly better than ultrasonic [4] | Potential for thermal effects or apical extrusion if improperly used [4] |
Each method comes with its own set of trade-offs. Ultrasonic activation is widely available and works well in straightforward cases, but its efficiency diminishes when the vibrating tip contacts canal walls – an issue particularly relevant in curved canals [5]. Multisonic systems stand out for their ability to clean complex root anatomies but require an investment in specialised equipment. Laser-activated irrigation offers comparable results to ultrasonic methods but demands careful training and equipment to ensure safe and effective use.
sbb-itb-2be92ed
Clinical Applications and Future Research
Clinical Relevance of Ultrasonic Activation
Passive Ultrasonic Irrigation (PUI) has proven to be more effective than traditional needle-and-syringe irrigation methods. Its ability to dynamically activate irrigants, particularly sodium hypochlorite (NaOCl), ensures better disinfection, especially in complex root canal anatomies [5]. PUI is often regarded as the go-to method for root canal disinfection, particularly for teeth with intricate structures. Traditional methods can leave behind residual bacteria in over 80% of cases, especially in the challenging apical region [3][5].
For optimal results, PUI relies on NaOCl concentrations between 1.5% and 3%, which effectively break down biofilms while minimising tissue damage [7]. Using saline alone, while it can dislodge bacteria, does not kill them [2]. To maximise the cleaning effect, clinicians are advised to move the ultrasonic file dynamically, as its disinfection impact is most effective within 1 mm of the vibrating tip [2].
New Research and Developments
Ongoing research is refining ultrasonic activation techniques to improve outcomes. For instance, studies using 3D-printed tooth models with standardised anatomies allow researchers to compare activation methods with greater precision and consistency [7]. This controlled approach helps evaluate key parameters, including activation duration, file positioning, and irrigant concentration.
Innovative technologies, like nanobubble water, are also gaining attention for their ability to enhance NaOCl penetration into dentinal tubules [7]. Additionally, combining ultrasonic activation with other disinfection strategies is showing promise – particularly in regenerative endodontics, where lower NaOCl concentrations are used to protect stem cells while still effectively targeting bacteria. Research from the University of Adelaide, published in the Australian Endodontic Journal, has shed light on how these advanced techniques perform in complex root systems [4]. These findings are helping to bridge the gap between laboratory research and practical application in clinical settings.
Applying Evidence-Based Practices in Australia
Australian dental professionals can incorporate ultrasonic activation into their regular practices by using protocols informed by the latest research. For effective apical cleaning, the ultrasonic tip should be positioned 1–2 mm short of the working length and activated for 30–60 seconds per canal. This approach not only improves cleaning but also minimises the risk of unnecessary dentine removal [5]. Clinics like Complete Smiles Bella Vista (https://completesmilesbv.com.au) can implement these evidence-based methods to enhance patient outcomes. It is essential that all clinical decisions adhere to AHPRA and Dental Board of Australia guidelines, ensuring treatment decisions are based solely on clinical necessity.
Conclusion
Passive Ultrasonic Irrigation (PUI) has been shown to outperform syringe irrigation in removing biofilm during root canal therapy. Research highlights that in simulated curved canals, using a flexible Nickel-Titanium tip positioned within 2 mm of the apex, PUI can achieve biofilm removal rates as high as 99.40% [6]. This effectiveness is attributed to acoustic streaming and cavitation, which disrupt bacterial clusters in hard-to-reach areas like lateral canals [1][6]. While these findings point to its potential, careful consideration is needed before fully integrating PUI into clinical practice.
For Australian dental professionals, it’s important to recognise the limitations of current evidence. Laboratory results showing high cleaning efficacy often differ from clinical outcomes. For example, studies reveal that 88% of mandibular molar roots still contain residual bacteria after treatment [2]. The cleaning effect diminishes significantly just 0.5 mm beyond the file tip [2], and bacterial regrowth can occur within five days [5]. Additionally, ultrasonic activation alone, especially with non-antimicrobial solutions, cannot achieve complete biofilm removal [2].
Another challenge lies in the inconsistency of research methodologies. Biofilm incubation periods in studies vary widely, from 1 to 50 days, making comparisons difficult [1]. Furthermore, newer technologies, such as multisonic systems, have shown better cleaning capabilities in complex canal anatomies than traditional PUI [3]. As a result, ultrasonic activation should be considered an adjunct to chemomechanical debridement rather than a standalone treatment.
To enhance clinical outcomes, practitioners should incorporate ultrasonic activation with sodium hypochlorite at effective concentrations, maintain dynamic file movement, and position the tip as close to the working length as possible [2][6]. Tailoring treatment protocols to the complexity of each case ensures a more evidence-based approach, ultimately supporting better patient outcomes in Australian dental practice.
FAQs
What makes ultrasonic activation more effective than traditional syringe irrigation for removing biofilm during root canal therapy?
When it comes to removing biofilm during root canal treatments, ultrasonic activation outperforms traditional syringe irrigation. Studies reveal that passive ultrasonic irrigation (PUI) not only allows irrigants to penetrate deeper into the canal system but also disrupts biofilm more effectively. This is largely thanks to the acoustic streaming and cavitation effects produced by the vibrating ultrasonic file. These mechanisms work together to dislodge bacteria and debris far more efficiently than what can be achieved with a syringe.
Traditional syringe irrigation often struggles to eliminate bacterial colonies hidden in hard-to-reach areas of the canal. In contrast, ultrasonic activation improves disinfection throughout the entire canal system, ensuring a more thorough cleaning process. This enhanced ability to remove biofilm underscores the benefits of ultrasonic techniques in improving the success rates of root canal treatments.
What challenges does ultrasonic activation face in cleaning curved root canals?
Ultrasonic activation works well to disrupt biofilm by generating acoustic streaming and shear forces, but its effectiveness drops in curved root canals. The vibrating file’s impact is strongest within about 1 mm of its tip, meaning areas beyond this range – particularly in the apical third – are often less thoroughly cleaned. The natural curve of the canal further complicates the process, as it limits the file’s ability to reach recessed walls while maintaining proper oscillation.
In curved canals, the file frequently makes contact with the outer wall at the bend. This contact dampens its vibrations and reduces the high-energy fluid motion needed to push the irrigant into less accessible parts of the canal. As a result, biofilm in these challenging regions may remain intact. To overcome this limitation, clinicians often pair ultrasonic activation with other techniques, such as gentle instrumentation or supplementary systems, to achieve a more complete cleaning of the canal system.
What are some alternatives to ultrasonic activation for biofilm removal during root canal therapy?
There are various effective methods for biofilm removal in root canal therapy that can serve as alternatives to ultrasonic activation. One option is sonic activation, which utilises a flexible tip vibrating at lower frequencies. When operated at higher power settings, it can deliver comparable results to ultrasonic techniques. Another advanced approach is multisonic systems, such as the GentleWave® platform, which combines acoustic energy with fluid dynamics to enhance biofilm removal in certain cases.
Laser-assisted irrigation is also a strong contender. Techniques like Er:YAG lasers are highly effective in eliminating biofilms and can be used either alongside or as a substitute for ultrasonic methods.
For a more traditional approach, manual syringe irrigation remains a dependable choice, particularly when the needle is placed close to the working length. This method can be further improved with specialised tips that create fluid agitation without relying on ultrasonic frequencies. Dentists often mix and match these techniques to ensure effective disinfection, adapting their approach based on the specific case and the tools at their disposal.
Related Blog Posts
- Benefits of Ultrasonic Activation in Dentistry
- Heat vs. Ultrasonic Tools in Root Canal Therapy
- Passive Ultrasonic Irrigation: Faster Root Canal Cleaning
- Sonic vs. Ultrasonic: Root Canal Cleaning Comparison
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





