







TMJ Anatomy: Key Components
The temporomandibular joint (TMJ) is a complex structure that enables essential functions like chewing, speaking, and breathing. It connects the lower jaw (mandible) to the temporal bone of the skull and is unique because it acts as both a hinge and a sliding joint. Here’s a quick breakdown of its key components:
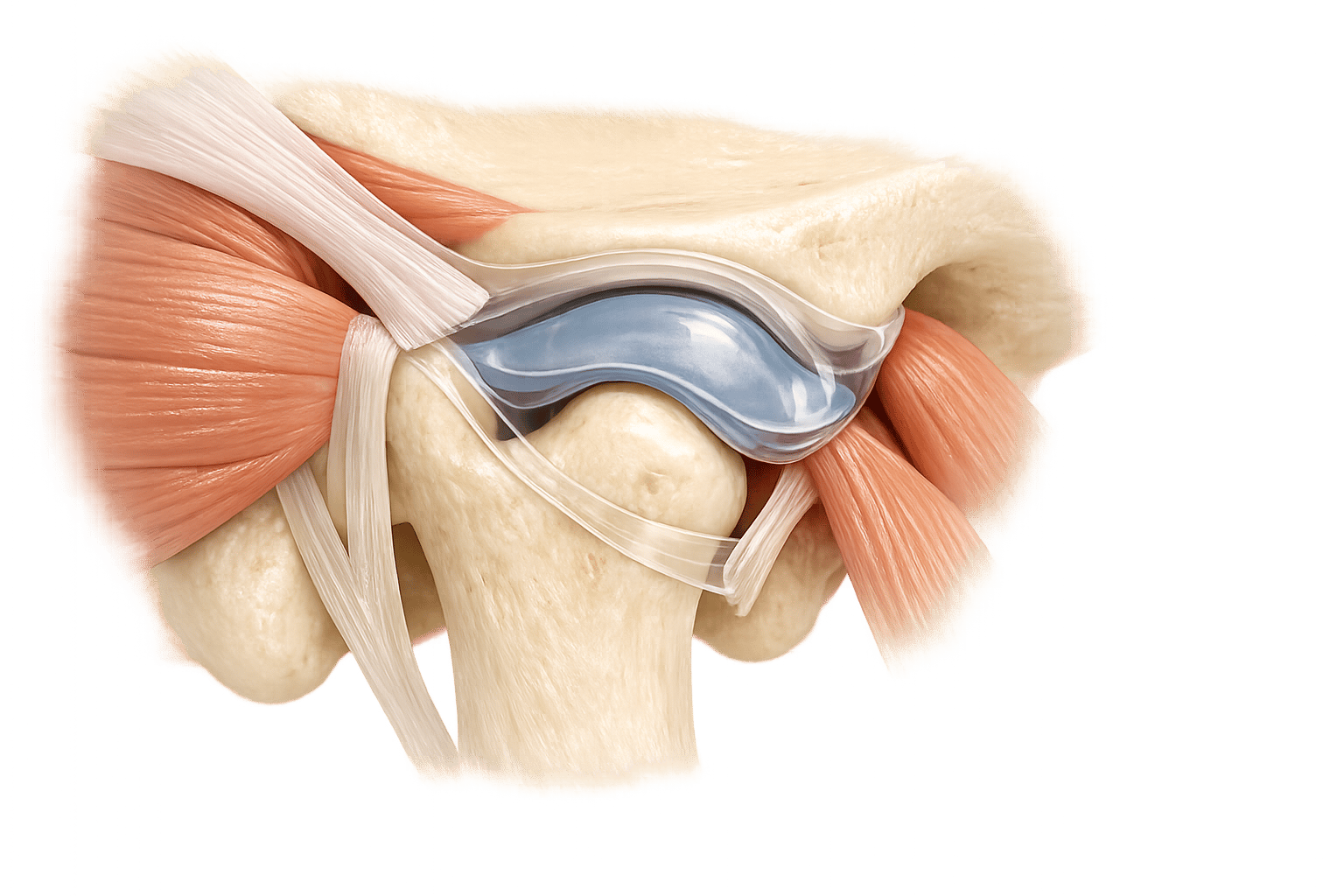
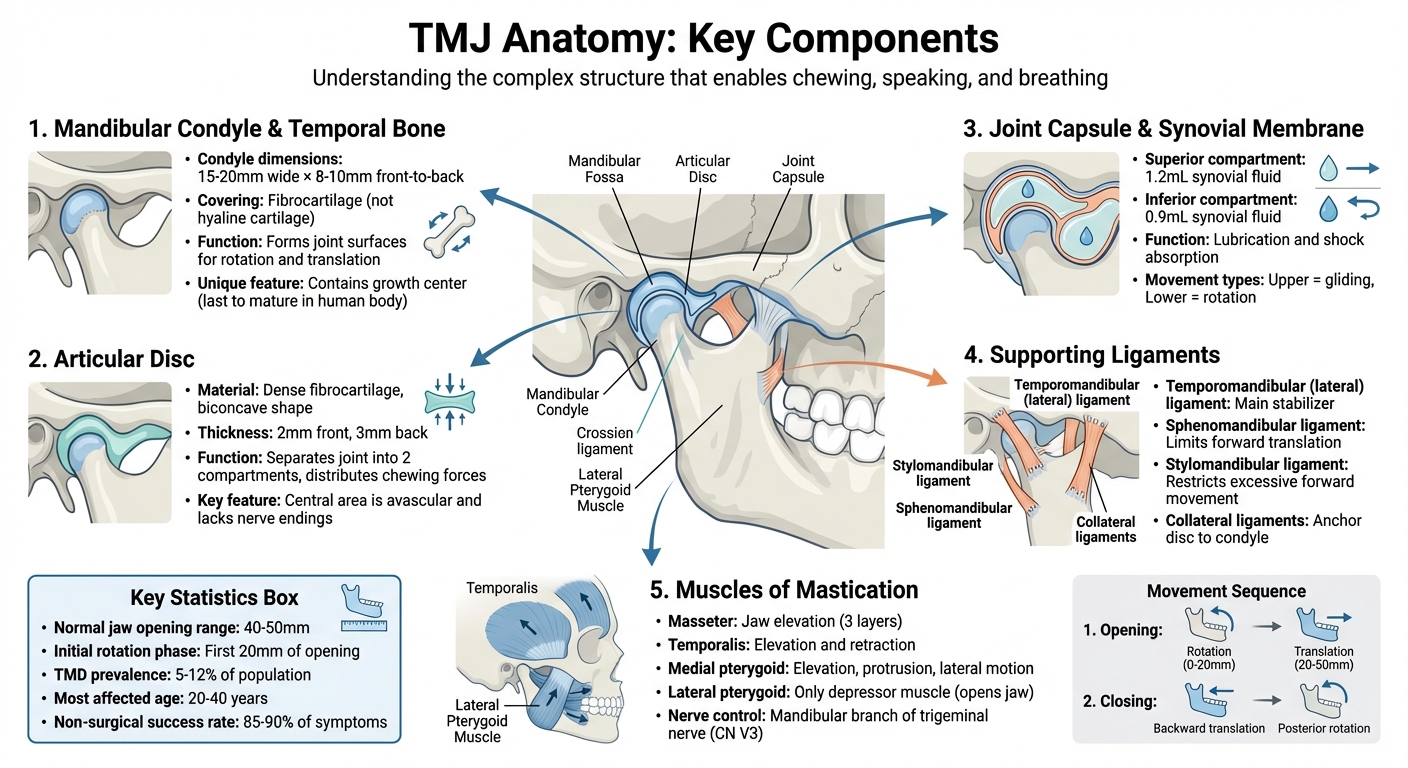
- Mandibular Condyle & Temporal Bone: These bony structures form the joint surfaces, covered in durable fibrocartilage for resilience during jaw movements.
- Articular Disc: A fibrocartilage separator that divides the joint into two compartments, allowing for smooth rotational and gliding motions.
- Joint Capsule & Synovial Membrane: Surrounds the joint, producing synovial fluid for lubrication and shock absorption.
- Ligaments: Provide stability and prevent excessive movement, including the lateral, sphenomandibular, and stylomandibular ligaments.
- Muscles of Mastication: Four key muscles (masseter, temporalis, medial pterygoid, and lateral pterygoid) control jaw movements like opening, closing, and grinding.
The TMJ’s unique anatomy allows for a jaw opening range of 40–50 mm and plays a critical role in daily activities. Understanding these components is vital for diagnosing and managing TMJ disorders, which affect 5–12% of people, especially between ages 20–40. Fortunately, non-surgical treatments effectively address 85–90% of symptoms.
If you experience jaw pain, clicking, or restricted movement, consult a professional for early diagnosis and care through our general dental services.
TMJ Anatomy: 5 Key Components and Their Functions
Temporomandibular Joint (TMJ) Anatomy | 3D Anatomy Tutorial | UKMLA | CPSA | PLAB 2
sbb-itb-2be92ed
1. Mandibular Condyle and Temporal Bone Surfaces
The temporomandibular joint (TMJ) is made up of two key bony structures: the mandibular condyle, which is part of the lower jaw, and the articular surfaces of the temporal bone, located in the skull. The mandibular condyle, a rounded head at the back of the mandibular ramus, typically measures about 15–20 millimetres across and 8–10 millimetres from front to back [4][1]. This structure forms the lower articulating surface of the TMJ.
The temporal bone contributes the upper portion of the joint through two main surfaces: the mandibular fossa (or glenoid fossa) and the articular eminence. The mandibular fossa is a concave area that holds the condyle when the jaw is at rest. The articular eminence, on the other hand, is a convex slope positioned in front of the fossa. This slope is essential for guiding the mandible’s forward and downward motion during activities like wide jaw opening [2].
Unlike many other joints, the TMJ’s articular surfaces are covered in fibrocartilage instead of hyaline cartilage [5][4][3]. Fibrocartilage is particularly well-suited to the TMJ’s demands, as it offers better regenerative capabilities and is more resistant to the complex forces created by chewing and speaking.
The interaction between these surfaces allows the TMJ to perform two main types of movement: rotation and translation. Rotation occurs in the lower joint compartment, functioning like a hinge, while translation happens in the upper compartment as the condyle glides along the articular eminence [2][4][1]. During the initial phase of mouth opening – roughly the first 20 millimetres – the condyle rotates against the articular disc [4][7]. As the jaw opens further, the condyle-disc complex moves forward and downward along the articular eminence.
Interestingly, the head of each mandibular condyle contains a growth centre that remains active until the body reaches full maturity. This growth centre is the last bone growth site to mature in the human body [4]. Its activity allows the mandible to lengthen, accommodating the development of permanent teeth and adult facial proportions.
Next, we’ll explore the articular disc and its role in TMJ function.
2. Articular Disc
The articular disc, made of dense fibrocartilage, sits snugly between the mandibular condyle and the temporal bone, forming a biconcave shape [9][2][4]. This disc serves as a separator, dividing the temporomandibular joint (TMJ) into two distinct synovial cavities: the upper (superior) compartment, located between the disc and the temporal bone, and the lower (inferior) compartment, positioned between the disc and the condyle [8][2][4]. These compartments have specific roles – the upper compartment allows for gliding (translational) movements, while the lower enables rotational, hinge-like motions [2][4].
The disc itself is elliptical, with a thinner middle zone and thicker edges, measuring approximately 2 mm at the front and 3 mm at the back [1]. This unique shape helps distribute chewing forces over a larger area, reducing stress on the underlying bones [2]. Essentially, the disc acts as a shock absorber, protecting the joint during biting and chewing.
Interestingly, the disc’s central area is avascular and lacks nerve endings, allowing it to endure compressive forces without triggering pain [2][4]. Instead of a direct blood supply, nutrients are delivered to the disc through the surrounding synovial fluid [4]. However, the retrodiscal tissue (also called the bilaminar zone) located behind the disc is highly vascular and innervated [8][2]. This makes it a common source of TMJ pain, especially when compressed due to disc displacement.
The disc is anchored medially and laterally to the condyle by collateral ligaments. It also connects anteriorly to the joint capsule and the superior head of the lateral pterygoid muscle, while posteriorly, it attaches to the temporal bone via the retrodiscal tissue [8][9][1][4]. These attachments ensure the disc moves in sync with the condyle during jaw activity.
As we age, the disc may thin, and its central portion can develop cartilage, which may interfere with smooth joint movement [4]. This wear and tear, combined with the disc’s critical role in maintaining proper alignment between the condyle and temporal bone [9][2], underscores just how essential the disc is for pain-free jaw function. Up next, we’ll look at the joint capsule and synovial membrane, which also play key roles in TMJ stability and movement.
3. Joint Capsule and Synovial Membrane
The TMJ’s capsule is a thin, fibrous covering that surrounds the joint. It connects to the mandibular fossa and articular tubercle at the top, and to the condylar neck at the bottom. This flexible structure allows for the wide range of movements required for activities like chewing, speaking, and yawning. Inside this capsule, the synovial membrane plays a key role.
Alongside the articular disc, the capsule creates the upper and lower joint compartments. It is highly innervated, providing essential feedback about jaw position and movement.
The synovial membrane, which lines the inside of the capsule (excluding the articular disc and condylar cartilage), produces synovial fluid. This fluid acts as a lubricant and shock absorber, ensuring smooth rotational and gliding motions of the joint.
When the capsule becomes inflamed, as in cases of capsulitis, it can thicken, causing pain, stiffness, and limited movement. This highlights how crucial a healthy joint capsule and synovial membrane are for comfortable and effective jaw function.
4. Supporting Ligaments
When it comes to the temporomandibular joint (TMJ), ligaments play a crucial role in stabilising and guiding its movement. These fibrous bands work in harmony to restrict excessive motion, protecting the joint and surrounding tissues from potential damage. Let’s take a closer look at the primary and supporting ligaments that keep the TMJ secure.
The temporomandibular (lateral) ligament is the main stabiliser of the TMJ. This thickened part of the lateral joint capsule stretches from the zygomatic process and articular tubercle to the neck of the mandibular condyle. It has two distinct components: an outer oblique portion and an inner horizontal portion. Together, these parts prevent excessive backward movement of the mandible while safeguarding the vascular and neural tissues beneath.
In addition to the primary ligament, there are two accessory ligaments that provide extra support:
- The sphenomandibular ligament connects the spine of the sphenoid bone to the lingula of the mandible. This ligament, a remnant of embryonic Meckel’s cartilage, acts like a hinge during jaw movement. It becomes especially important after the first 10° of mouth opening, helping to limit excessive forward translation of the mandibular condyle.
- The stylomandibular ligament, a thickened band of deep cervical fascia, runs from the styloid process to the angle and posterior edge of the mandible. Its primary role is to restrict excessive forward movement of the jaw.
Another key component is the collateral (discal) ligaments, which anchor the articular disc to the medial and lateral poles of the mandibular condyle. These ligaments ensure the disc and condyle move together as a single unit, maintaining proper alignment during jaw movements.
Interestingly, the ligaments of the TMJ also contain mechanoreceptors, which send proprioceptive signals to the central nervous system. This feedback is vital for coordinating smooth and controlled jaw movements. However, injuries or excessive strain – such as from trauma or overextension – can lead to ligament laxity. This instability may cause issues like clicking sounds or even displacement of the articular disc, affecting overall joint function, which may require general dental treatments to manage.
5. Muscles of Mastication and Lateral Pterygoid
The temporomandibular joint (TMJ) depends on four main muscles of mastication: the masseter, temporalis, medial pterygoid, and lateral pterygoid. All of these muscles are controlled by the mandibular branch of the trigeminal nerve (CN V3). Together, they ensure smooth chewing, speaking, and jaw movements.
The masseter, temporalis, and medial pterygoid primarily function as elevator muscles, responsible for closing the jaw. The masseter, a rectangular muscle with three layers, originates from the zygomatic arch and attaches to the mandibular ramus. The temporalis, shaped like a fan, has vertical fibres that elevate the jaw and horizontal posterior fibres that retract it, aiding in positioning the condyle-disc complex. Working alongside the medial pterygoid, the masseter forms the pterygomasseteric sling, which plays a key role in jaw elevation, protrusion, and lateral motion during chewing.
The lateral pterygoid, however, stands out as the only mastication muscle that depresses the mandible, allowing the jaw to open. This muscle has two distinct heads: the superior head connects to the TMJ’s articular disc and capsule, while the larger inferior head (roughly three times the size) attaches to the pterygoid fovea on the mandibular condyle [11][10]. This structure enables smooth disc-condyle coordination. When both heads contract simultaneously, the mandible protrudes. Unilateral contraction, along with the medial pterygoid, produces lateral movements crucial for the grinding phase of chewing.
Dysfunction in these muscles, particularly the lateral pterygoid, can lead to TMJ disorders. Issues like spasms or poor coordination between the two heads of the lateral pterygoid can result in anterior disc displacement, often causing clicking sounds or limited jaw movement. Interestingly, the lateral pterygoid is unique among the mastication muscles as it lacks muscle spindles (stretch receptors), which may explain its specialised role in detecting changes in muscle length [10][11].
Next, we’ll delve into the joint compartments and their importance in jaw movement.
6. Joint Compartments and How the Jaw Moves
The muscles of mastication work in harmony with the temporomandibular joint (TMJ), and understanding the TMJ’s joint compartments sheds light on how the jaw achieves its precise movements.
The TMJ is divided by the articular disc into two distinct synovial cavities: the superior (discotemporal) and inferior (discomandibular) compartments. These compartments are normally separate unless the disc sustains damage, which could allow communication between them [4].
Each compartment has a specialised function. The inferior compartment is responsible for rotational, hinge-like movements, which are key to the initial phase of opening the mouth. On the other hand, the superior compartment handles translational, gliding movements, enabling actions like protrusion and retraction of the jaw [4]. The superior compartment contains about 1.2 mL of synovial fluid, while the inferior holds approximately 0.9 mL [3].
When opening the mouth, the process begins with about 20 mm of rotation within the inferior compartment. After this, the disc-condyle complex moves forward and downward along the articular eminence, allowing for a full jaw opening of 40–50 mm [4][6]. The lateral pterygoid muscle plays a key role here: its superior head guides the translational movement, while its inferior head manages the rotational phase [6].
Closing the jaw reverses this sequence. It starts with a backward translation in the superior compartment, followed by a posterior rotation in the inferior compartment [6]. While rotation is dominant in the early stages of opening, and translation takes over later, these movements often occur together during activities like chewing and speaking [3].
Clinical Applications
Precise knowledge of the temporomandibular joint (TMJ) structure plays a significant role in diagnosing and treating temporomandibular disorders (TMD). This understanding helps clinicians accurately identify pain sources and implement targeted treatments, as highlighted earlier.
A key aspect of TMJ anatomy is recognising the difference in sensitivity between various components. For example, while the central articular disc lacks nerve supply, the surrounding retrodiscal tissue and joint capsule are highly sensitive. This explains why even minor disc displacements can lead to significant discomfort – compressed or inflamed retrodiscal tissues are major contributors to TMJ-related pain [6].
Another critical factor is the relationship between the mandibular condyle and the articular disc. This knowledge allows practitioners to differentiate between disc displacement with reduction (often accompanied by clicking or popping sounds as the condyle repositions onto the disc) and displacement without reduction, which can result in restricted jaw movement or a locked jaw [6]. Additionally, understanding the TMJ’s two-compartment system – where rotation occurs in the lower compartment and translation in the upper compartment – enables clinicians to identify which phase of movement is impaired during jaw opening or closing [6][3].
Since the TMJs work in tandem, identifying how an asymptomatic joint might affect a symptomatic one is crucial. Dysfunction in one joint often leads to compensatory issues in the other, complicating the overall condition [6]. Encouragingly, most TMJ disorder symptoms – approximately 85% to 90% – can be addressed through noninvasive treatments like manual therapy, splints, and targeted exercises [1].
At Complete Smiles Bella Vista, Dr. James Hanna and his team use their advanced understanding of TMJ anatomy to provide precise diagnoses and evidence-based treatments, ranging from conservative therapies to specialised interventions.
Conclusion
The temporomandibular joint (TMJ) plays a crucial role in essential functions like speaking, chewing, and yawning. Its operation depends on the interaction between the mandibular condyle and the temporal bone, supported by the joint capsule, ligaments, and muscles of mastication. These components work together to provide stability and control, allowing for a jaw opening range of approximately 40–50 millimetres [4]. This precise coordination is key to diagnosing and managing TMJ disorders effectively.
"Sound knowledge of anatomy is essential and an appreciation of the anatomical features associated with the TMJ can serve as a foundation for understanding the clinical management of temporomandibular disorders." – British Dental Association [12]
A clear understanding of these anatomical elements is vital for dental professionals when making clinical decisions about temporomandibular disorders (TMD). With TMD affecting an estimated 5–12% of the population [6], recognising that even an asymptomatic joint can sometimes contribute to dysfunction helps clinicians pinpoint pain sources and choose the best treatment options.
If you’re dealing with jaw clicking, locking, persistent facial pain, or restricted movement, it’s important to consult a dental professional. The good news is that around 85–90% of TMJ disorder symptoms can be addressed with noninvasive, nonsurgical treatments [1], making early diagnosis and care essential for effective relief.
FAQs
What’s the difference between TMJ rotation and translation?
The TMJ enables two key types of movement: rotation and translation. Rotation happens when the mandibular condyle pivots around a fixed point, similar to how a hinge works. This movement is most noticeable during the initial stages of opening or closing the mouth. Translation, on the other hand, involves the condyle gliding forward or backward along the articular eminence, which allows for wider jaw openings. These movements don’t work in isolation – rotation is more prominent in the early phases, while translation takes over to provide a greater range of motion.
Why does the TMJ click or pop when I open my mouth?
When you open your mouth, the TMJ (temporomandibular joint) might make a clicking or popping sound. This happens because the articular disc – a small, cushion-like structure in the joint – can briefly slip out of its usual position, moving in front of the condylar head. As the disc shifts back into place, it creates the sound. This is a fairly common occurrence and is often just a normal part of how the joint operates.
When should I see a dentist about TMJ pain or locking?
If you’re dealing with persistent TMJ pain or your jaw frequently locks, it’s time to see a dentist. These could be signs of a condition that needs professional attention. Getting it checked early can ease the discomfort and help avoid potential issues down the track.
Related Blog Posts
- Advances in Sleep Studies for Orofacial Pain
- EMG Biofeedback for TMJ Disorders: What to Know
- Best Sleep Positions for Jaw Pain Relief
- How Aligners Move the Jaw
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





