







How Aligners Move the Jaw

Aligners work by applying gentle, consistent pressure to teeth, gradually shifting them into new positions. These clear, removable trays use advanced materials like TPU and PETG to deliver precise forces. Each aligner moves teeth by about 0.2–0.25 mm, relying on the body’s natural bone remodelling process. This involves breaking down bone on one side of a tooth and forming new bone on the other. While aligners are effective for many cases, they can struggle with complex movements like deep bite correction or molar extrusion. Tools like attachments, elastics, and temporary anchorage devices (TADs) are often added to enhance results. However, patient compliance – wearing aligners for 20–22 hours daily – is key to success.
Key Points:
- Aligners apply pressure to move teeth gradually.
- Bone remodelling supports this process, with changes beginning within 24–48 hours.
- Attachments and elastics improve precision for difficult cases.
- Aligners are less effective for complex movements like deep bite correction.
- Consistent wear is essential for effective results.
The Biomechanics Behind Aligner Therapy
How Aligners Apply Force
Clear aligners work by using their elastic properties to gently push teeth into the desired position. When placed on the teeth, the aligner material naturally tries to return to its original shape, creating controlled pressure on the teeth [3].
This pressure comes from the mismatch between the aligner’s pre-designed shape and the current position of the teeth. Advanced digital designs ensure the aligners apply precise 3D forces to specific contact points [4].
The materials used – most commonly thermoplastic polyurethane (TPU) or polyethylene terephthalate glycol (PETG) – play a critical role in how the force is delivered. Factors like elasticity, stress relaxation, and creep behaviour influence how pressure is applied. Research indicates that effective tooth movement occurs when the periodontal membrane experiences hydrostatic pressure between 4.7 and 16 KPa [3]. To achieve this, aligners are typically designed with an activation range of 0.2 to 0.5 millimetres per stage [3].
Advanced 3D modelling further refines this process, ensuring that forces are distributed accurately for precise tooth movement.
3D Modelling and Force Distribution
Digital simulations, such as those using Finite Element Analysis (FEA), allow orthodontists to visualise stress patterns and predict tooth displacement. These models identify each tooth’s centre of resistance, which is usually located about two-fifths of the distance from the alveolar ridge crest. This is vital for achieving controlled tooth movement and avoiding unwanted tipping [6][5].
3D modelling also helps optimise "torque compensation", a design feature that counteracts unintended movements. For example, during mandibular advancement, aligners incorporate torque compensation angles of 15°–20° to prevent labial tipping of the lower central incisors [2]. Even small design choices, like trimming styles, can have a noticeable impact. Straight trimming lines, for instance, generate higher active and passive pressures compared to scalloped designs [3].
That said, clear aligners are not perfect. Studies show that their overall tooth movement accuracy is around 56.18%. Mesiodistal movements are the most accurate at 72.33%, while intrusion movements are less predictable, with an accuracy of only 43.28% [6].
Aligners Biomechanics: How Do Clear Aligners Move Teeth?
Biological Process of Jaw Movement
How Dental Aligners Move Teeth: The Bone Remodeling Process
Bone Remodelling and Cellular Activity
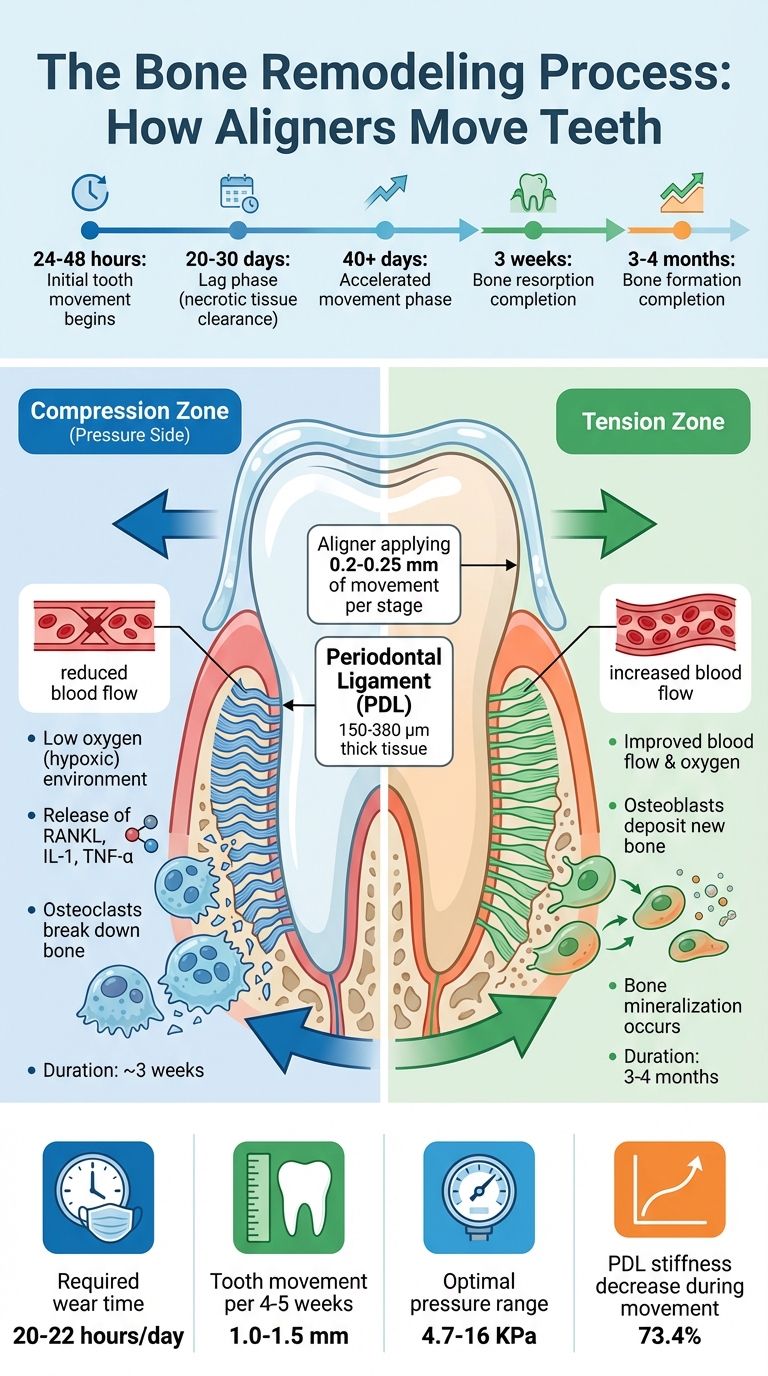
Aligners work by applying pressure to your teeth, setting off a biological process called the pressure-tension mechanism. This creates two distinct zones: compression, where bone is resorbed, and tension, where new bone is deposited [7][8].
On the compression side, reduced blood flow creates a low-oxygen (hypoxic) environment. This triggers the release of inflammatory molecules like RANKL, IL-1, and TNF-α, which recruit osteoclasts to break down bone. This bone resorption stage takes roughly three weeks, allowing space for teeth to move [9].
On the tension side, the stretching of periodontal ligament fibres improves blood flow and oxygen levels. This activates osteoblasts, which deposit mineralised bone to stabilise the tooth in its new position. However, this bone formation process is slower, often taking three to four months [7][9].
Tooth movement starts within 24 to 48 hours of applying force. It then enters a lag phase of 20 to 30 days, during which necrotic tissue is cleared. After about 40 days of continuous force, the pace of movement increases significantly [7].
Osteocytes, the cells embedded within the bone, play a key role in this process. They act as mechanosensors, detecting changes in fluid flow within bone canaliculi and signalling osteoblasts and osteoclasts where remodelling is needed. The periodontal ligament is central to this process, acting as the pathway for these mechanical forces.
Role of the Periodontal Ligament
The periodontal ligament (PDL) is essential in transferring the stress from aligners to the surrounding bone. This connective tissue, which is 150–380 µm thick, not only senses mechanical strain but also cushions the tooth against trauma [8][10].
Structurally, the PDL forms a fibrous connection between the tooth and the alveolar bone, creating a functional joint [8]. Within the PDL, fibroblasts detect strain through focal adhesion complexes. These complexes transmit mechanical signals to the nucleus, triggering gene expression that starts the bone remodelling process [10]. Additionally, the PDL controls the RANKL/OPG ratio. At compression sites, PDL cells increase RANKL production, which stimulates osteoclast activity for bone resorption [11][10].
"The periodontal ligament and alveolar bone make up a functional unit that undergoes robust changes during orthodontic tooth movement." – Jaap C. Maltha, Department of Dentistry – Orthodontics and Craniofacial Biology [10]
When optimal force is applied, teeth move at a rate of about 1.0 to 1.5 millimetres every four to five weeks [11]. However, applying too much force can lead to PDL hyalinisation – a sterile necrosis caused by trauma. In such cases, tooth movement halts temporarily until macrophages clear the necrotic tissue [11][10]. Studies also reveal that PDL stiffness can decrease by as much as 73.4% during orthodontic movement [8].
sbb-itb-2be92ed
Tools and Techniques for Enhanced Jaw Movement
Attachments and Pressure Points
Aligners can sometimes struggle with precision, especially in more complex orthodontic cases. To address this, orthodontists use small, tooth-coloured composite resin structures bonded to the teeth, known as attachments. These attachments act like handles, giving the aligner a specific surface to apply force. Essentially, they help increase the contact area and adjust force directions, making them especially handy for preventing aligners from slipping over rounded teeth during rotations.
Each attachment has three parts: an active surface, a passive surface, and a base. Placement is key – positioning an attachment further from the tooth’s centre of resistance creates a stronger rotational effect. For instance, studies show molar distalisation achieves about 88.4% accuracy when attachments are used [13].
"Attachments mostly increase the effectiveness of orthodontic treatment with clear aligners, improving anterior root torque, rotation, and mesio-distal (M-D) movement; they are also important to increase posterior anchorage." [13]
The process of applying these attachments takes roughly 30 minutes. To ensure the aligner works effectively and avoids deformation, attachments should be placed at least 1.5 millimetres from the gingival margin [12].
These attachments often work alongside other tools to handle cases requiring more complex force applications. Together with digital treatment planning, they ensure forces are applied with precision.
Use of Elastics and Temporary Anchorage Devices (TADs)
Attachments are just the start – auxiliary devices like elastics and temporary anchorage devices (TADs) take jaw movement to the next level in more challenging cases. For major inter-arch corrections, like those seen in Class II or Class III malocclusions, these tools provide extra support. Intermaxillary elastics, for example, help align the upper and lower jaws. However, since elastics can sometimes pull the aligner out of place vertically, orthodontists often bond additional retentive attachments to nearby teeth to keep everything secure.
TADs, on the other hand, offer a fixed point of anchorage, providing unmatched stability. This makes them ideal for complex movements like molar distalisation or tooth intrusion, as they can prevent unwanted shifts in neighbouring teeth. Without these auxiliary supports, certain movements – like rotating a tooth – might only achieve partial results. For instance, without proper support, only 35 out of 45 degrees of planned rotation might be achieved [14].
"To mitigate the biomechanical limitations of aligners, particularly in complex cases, additional methods – such as attachments, buttons, power arms, precise cuts on the aligners, bite ramps, temporary anchorage devices, and intermaxillary elastics – are often employed." [12]
One notable difference between elastics and TADs is patient involvement. Elastics require daily replacement by the patient, making compliance essential. TADs, however, stay fixed and provide consistent force under the clinician’s control, requiring no extra effort from the patient. Both tools, when used effectively, can make a significant difference in achieving desired outcomes.
Effectiveness and Limitations of Aligners for Jaw Alignment
Research on Predictability of Tooth and Jaw Movement
Studies suggest that aligners perform variably across different types of dental movements. For instance, expansion movements show over 75% accuracy, while incisor rotations fall between 50% and 75%. However, more challenging movements like canine or premolar rotations, as well as extrusion and intrusion, often achieve less than 50% accuracy [15]. On average, the predictability of dental movement using aligners ranges from 55% to 72%. When it comes to rotational movements, the mandibular arch tends to perform slightly better, with an accuracy of about 78.6%, compared to 75.0% in the maxillary arch [17].
Deep overbite correction remains particularly difficult, with aligners achieving only 39% to 52% of the digitally predicted bite opening [21].
"One of the most commonly reported clinical concerns with CAT is the discrepancy between the prescribed outcome in the digital treatment plan and the clinically achieved outcome." – Yashodhan M. Bichu, University of British Columbia Faculty of Dentistry [21]
Aligner therapy generally takes less time, averaging 13.35 months compared to 19.08 months for fixed braces. However, over 70% of aligner cases require at least one refinement stage [16][22]. Despite their efficiency, aligners are less effective for complex malocclusions, as shown by lower Peer Assessment Rating (PAR) index scores compared to fixed appliances [16]. These findings underline the limitations of aligners in achieving certain advanced movements.
Limitations of Aligner Therapy
Deep bite correction is a notable weak point for aligners, with less than 50% of the planned overbite reduction typically achieved. The plastic material of aligners often creates a "bite-block" effect, leading to posterior open bites or loss of occlusal contacts [20][21][18]. Similarly, molar extrusion, which is crucial for some jaw corrections, only achieves 30–40% of the planned movement [20]. These biomechanical limitations highlight the need for additional tools and careful treatment planning.
The anatomy of certain teeth also poses a challenge. Canines and premolars, with their rounded shapes, are harder for aligners to grip, resulting in rotational accuracy as low as 36% for canines. Second molars often show the lowest accuracy in both arches due to factors like inadequate distal anchorage and shorter crowns [19][17]. Achieving complex movements such as significant root torque or bodily tooth movement remains difficult with aligners, which are better suited for simpler tipping movements [21][18].
Patient compliance is another critical factor. Only about 36% of patients adhere fully to the recommended 22-hour daily wear time [23]. Additionally, severe spacing can increase the likelihood of treatment refinements by up to 20.9 times [23]. For more complex cases – such as severe crowding (over 6 millimetres), significant vertical discrepancies, or major root torque requirements – fixed appliances often provide better results [21].
These challenges stem from the biomechanical limitations and force distribution patterns inherent to aligners. To address these issues, clinicians frequently incorporate overcorrection into digital treatment plans, particularly for movements like transverse expansion and rotations, to account for the gap between planned and actual outcomes [21][18].
Conclusion
Orthodontic aligners work by combining physical forces with the body’s natural biological responses. They apply controlled pressure to tooth surfaces, prompting a cascade of activity within the periodontal ligament. This process triggers bone remodelling: osteoclasts break down bone tissue on the pressure side, while osteoblasts build new bone on the tension side, allowing teeth and jaw structures to gradually shift into their desired positions [24].
The timeline of tooth movement follows a predictable pattern. Initial movement begins within 24–48 hours of applying force, followed by a lag phase lasting 20–30 days. Around day 40, the rate of movement picks up again as the remodelling process continues [7]. To sustain this biological activity, aligners must be worn consistently for 20–22 hours each day [1].
"The effectiveness of orthodontic tooth movement is directly correlated to the biology of tooth movement." – Dr. Tanya Prasa, BDS, MDS [4]
This quote highlights the critical role of biological processes in achieving successful outcomes with aligners.
That said, aligners do have limitations. They excel in predictable movements like expansion, achieving over 75% accuracy, but they often struggle with more complex adjustments. Movements such as extrusion, intrusion, and canine rotations typically achieve less than 50% of the planned results [15]. Deep overbite correction is particularly tough, with only 30–40% of planned molar extrusion being realised in many cases [20].
Because of these challenges, professional oversight is essential. A qualified clinician will assess factors like bone density, age, and oral health to determine whether aligners are the right choice for a patient [1]. For more complex movements, they may use additional tools such as attachments, elastics, or Temporary Anchorage Devices to improve force predictability [3][24]. Regular monitoring ensures that the treatment stays on track with the digital plan, allowing adjustments if needed.
For those exploring aligner therapy, Complete Smiles Bella Vista offers detailed orthodontic assessments, including Invisalign treatment planning, to help identify the best approach for each individual case.
FAQs
How do aligners move teeth using bone remodelling?
Aligners work by applying a gentle and consistent pressure to your teeth, stimulating the periodontal ligament that surrounds each one. This triggers a natural process known as bone remodelling. Here’s how it works: on the side of the tooth where pressure is applied (the compression side), bone tissue is broken down, while on the opposite side (the tension side), new bone tissue is formed. This coordinated process allows teeth to gradually shift into their proper positions.
The movement is carefully managed to ensure it happens slowly and safely, improving alignment while supporting your overall oral health.
Are there any limitations to how aligners can move the jaw?
While aligners work well for many orthodontic treatments, they do have their limits, especially when dealing with more complicated jaw movements. For instance, they can face challenges in achieving precise rotations, root uprighting, or specific torque movements. These issues are particularly common with premolars and canines, where the success rate of movement can sometimes drop to just 50–75%.
In such situations, other orthodontic tools or techniques might be necessary to get the desired results. Consulting an experienced orthodontist is crucial to determine if aligners are the right choice for your individual needs.
How do attachments and temporary anchorage devices (TADs) improve the effectiveness of aligners?
Attachments and temporary anchorage devices (TADs) play a crucial role in making aligners more effective by enabling precise and complex tooth movements.
Attachments are small, tooth-coloured shapes bonded directly to the teeth. These help aligners apply targeted forces for specific movements like rotations, extrusions, and torque adjustments. Each attachment is customised to the patient’s needs, ensuring better control and precision throughout the treatment.
TADs, on the other hand, serve as stable anchorage points. Unlike attachments, they don’t rely on neighbouring teeth for support. This makes them ideal for more challenging tasks, such as repositioning molars or correcting severe misalignments.
When combined with aligners, these tools help orthodontic treatments achieve more predictable outcomes, shorten treatment durations, and tackle a broader range of alignment issues effectively.
Related Blog Posts
- How Material Composition Affects Clear Aligner Performance
- Aligner Fit: Biomechanics Behind Edge Design
- How Orthodontic Forces Remodel Alveolar Bone
- Benefits of 3D-Printed Clear Aligners
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





