







Study: Accuracy of 10 Intraoral Scanners

Choosing the right intraoral scanner is critical for dental precision. A recent study compared 10 scanners used in Australia for full-arch impressions, focusing on accuracy metrics like trueness and precision. Key findings include:
- Top performers: CEREC Primescan and Trios 3, with minimal deviations (~140 μm).
- Mid-range options: Medit i700 and Dexis IS 3800W, suitable for simpler cases.
- Lower accuracy: DWIO and PlanScan, with deviations exceeding 300 μm.
- Full-arch challenges: Accuracy drops in longer scans, especially in vertical dimensions.
Laboratory conditions ensured controlled testing, but real-world factors like saliva and patient movement can significantly affect results. For Australian dentists, selecting a scanner depends on case complexity, with high-end models recommended for implants or full-arch work. Training and clinical considerations are equally important for achieving precise outcomes.
How the Study Was Conducted
Trueness and Precision Explained
When evaluating scanner performance, two key metrics come into play: trueness and precision. Simply put, trueness measures how closely a scanner’s digital impression aligns with a reference standard, essentially gauging its accuracy. As defined by ISO 5625-1, "Trueness refers to the level of agreement between the arithmetical mean of a large number of tests and the true or accepted value" [8].
Meanwhile, precision focuses on consistency. According to DIN ISO 5725-2, "Precision defines the congruence between multiple virtual casts of the same anatomic structure" [1]. In other words, precision tells you how much variation exists when the same model is scanned multiple times. A scanner could exhibit high precision but low trueness (consistently inaccurate) or high trueness but low precision (randomly accurate). These metrics are quantified using the Root Mean Square (RMS) error, which calculates the square root of the mean of squared deviations between the reference standard and the scan data points [2].
With these definitions in mind, let’s dive into the testing setup used to evaluate these metrics.
Testing Setup and Study Constraints
To ensure reliable and meaningful results, the study was conducted under tightly controlled conditions. High-precision reference standards were employed, including Coordinate Measuring Machines (CMM) with certified accuracy levels as precise as 3.5 μm [9]. Additionally, industrial-grade desktop scanners served as the benchmark, or "gold standard", for assessing intraoral scanner performance. The test models ranged from mandibular typodonts (artificial dental models) to edentulous models incorporating PEEK scan bodies. These materials were specifically chosen for their dimensional stability and ability to mimic clinical conditions [2][8][9].
Environmental conditions were carefully standardised. Ambient lighting was maintained at 1000 lux, reflecting typical room conditions optimal for most scanners [2][7]. However, it’s worth noting that these laboratory conditions don’t fully replicate real-world challenges. Clinical scanning often involves hurdles like saliva, patient movement, and operator variability – all of which can significantly affect results. For instance, research indicates that the presence of saliva and blood can lead to deviations that are 2–4 times higher than what is considered clinically acceptable [10].
The study also relied on advanced alignment methods to ensure accurate comparisons. The Iterative Closest Point (ICP) algorithm was used to superimpose scans for analysis [2][1]. The choice of software played a crucial role as well. For instance, Geomagic Control X, a tool widely used for 3D inspection and RMS error quantification, consistently produced lower RMS values compared to alternatives like MeshLab or CloudCompare [2]. Notably, accuracy improvements were found to plateau after aligning 20 points [2].
The No-Nonsense Guide to Intraoral Scanners
The 10 Intraoral Scanners Tested
This study evaluated a variety of intraoral scanners available in Australia, ranging from budget-friendly to high-end systems. These devices utilise technologies like confocal microscopy, active triangulation, or active wavefront sampling to capture data[2][8]. Most modern scanners are powder-free, but older models, such as True Definition, still require a titanium dioxide coating for scanning[8].
The scanners were chosen based on their popularity in Australian dental practices, their technological differences, and their relevance across various price ranges. Prices for these devices range from approximately A$7,000 to A$26,000. The selection includes major brands like Dentsply Sirona, 3Shape, Medit, and iTero, ensuring the study reflects clinical conditions commonly faced by practitioners[2][8]. Below are the performance results for each scanner tested.
Dexis IS 3800W Results
The Dexis IS 3800W (formerly CS 3600) uses active triangulation technology with video sequence capture[8]. When assessing its accuracy, the study noted that root mean square (RMS) deviation values varied depending on whether quadrant or full-arch scans were performed. Let’s move on to the results for other leading brands.
Medit i700 Results
The Medit i700, which also employs active triangulation with video sequence capture, showed solid accuracy for full-arch scans, particularly in partially edentulous cases[4][8]. Comparative studies ranked the i700 favourably for trueness, placing it between top-tier performers and mid-range options.
Primescan 2 Results
The CEREC Primescan, which combines confocal microscopy with high-frequency contrast analysis, emerged as one of the top performers in accuracy tests[2][8]. Trueness measurements for the Primescan were recorded at 142.04 μm, highlighting its strong performance in the study[8].
"The CEREC Primescan and Trios 3 had the highest trueness followed by i500, Trios 2, and iTero Element… and the DWIO and PlanScan had the lowest trueness." – Ryan Jin Young Kim, Researcher[8]
Trios 5 Results
The 3Shape Trios 5, which uses confocal microscopy with video sequence acquisition, operates without the need for powder[8]. The Trios series consistently delivers high precision in full-arch implant scans, making it highly suitable for complex restorative workflows[7].
Results for Remaining Scanners
Other scanners in the study were evaluated using the same rigorous criteria. The iTero Element employs parallel confocal microscopy, while the CEREC Omnicam uses active triangulation with stripe projection. True Definition relies on active wavefront sampling and requires a coating, while PlanScan utilises laser triangulation[2][8]. Among these, the DWIO and PlanScan recorded lower trueness values in partially edentulous scans compared to their competitors[8]. These findings contribute to the broader comparison of scanner accuracy.
Scanner Accuracy Comparison
Intraoral Scanner Accuracy Comparison: 10 Models Tested
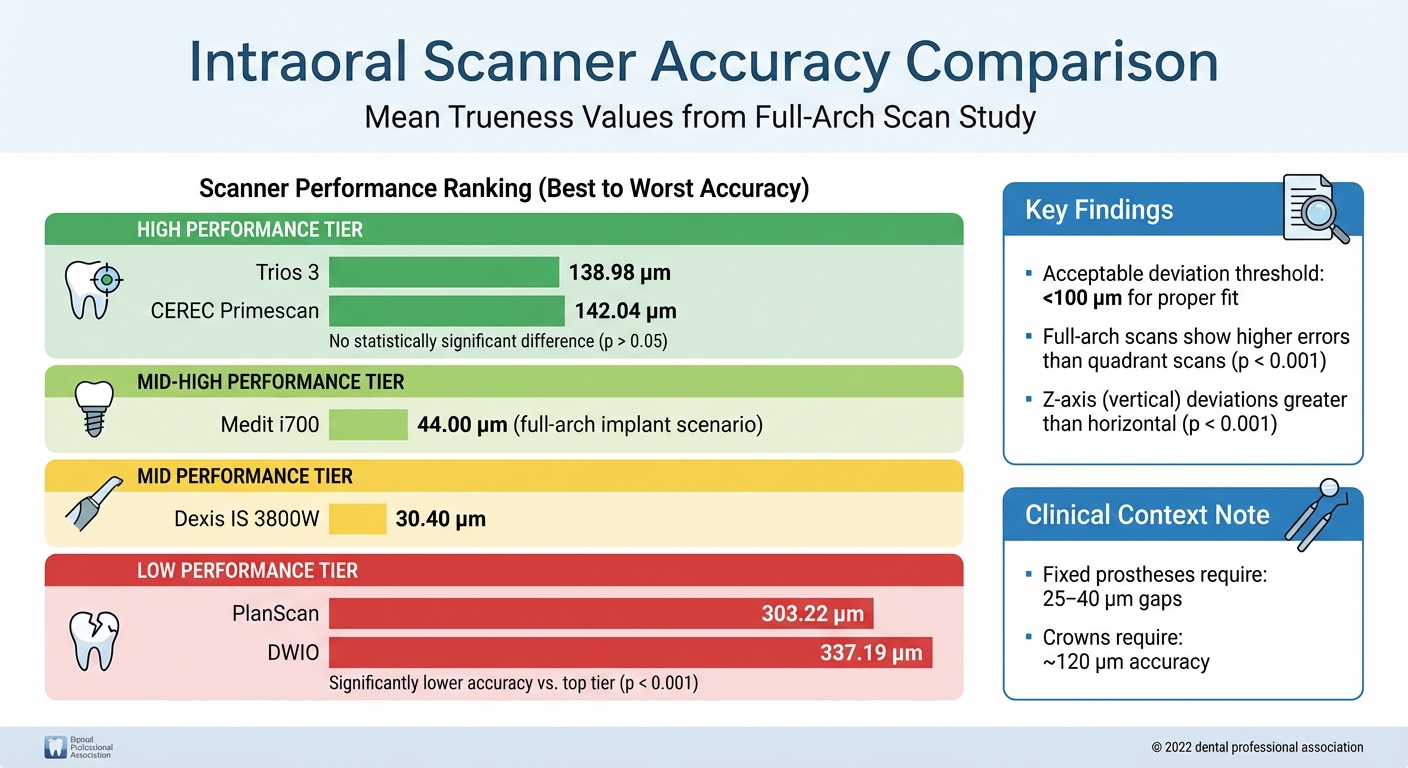
When comparing the accuracy metrics of 10 intraoral scanners, clear performance differences emerged. High-accuracy scanners displayed minimal deviations, while entry-level systems exhibited significantly larger errors. Among the top-tier scanners, the performance gap was relatively small.
The CEREC Primescan and Trios 3 demonstrated outstanding accuracy, with mean deviations of 142.04 μm and 138.98 μm respectively. The difference between these two was not statistically significant (p > 0.05) [8]. On the other hand, scanners like the DWIO and PlanScan showed much higher deviation values, at 337.19 μm and 303.22 μm respectively [8]. In full-arch implant scenarios, the Medit i700 achieved a trueness value of approximately 44 μm, placing it between the highest-performing and lower-performing groups [7]. The table below offers a closer look at the performance breakdown:
| Scanner Model | Mean Trueness (μm) | Statistical Significance | Performance Tier |
|---|---|---|---|
| Trios 3 | 138.98 | p > 0.05 vs Primescan | High |
| CEREC Primescan | 142.04 | p > 0.05 vs Trios 3 | High |
| Medit i700 | 44.00 | – | Mid-High |
| Dexis IS 3800W | 30.40 | – | Mid |
| PlanScan | 303.22 | p < 0.001 vs top tier | Low |
| DWIO | 337.19 | p < 0.001 vs top tier | Low |
Accuracy also declined as scanning distances increased. For example, full-arch scans resulted in significantly higher errors compared to quadrant or short-span scans (p < 0.001) [6]. Furthermore, deviations were typically more pronounced in the Z-axis (vertical dimension) than in horizontal planes (p < 0.001) [8].
sbb-itb-2be92ed
What the Results Mean for Australian Dentists
When it comes to dental restorations, precision is everything. For example, deviations in accuracy exceeding 100 μm can compromise the fit of restorations. Fixed prostheses typically require gaps of 25–40 μm, while crowns need around 120 μm [1][6][13]. These benchmarks explain why choosing the right scanner is so critical, especially for intricate cases like full-arch rehabilitations or implant-supported prostheses.
Selecting a scanner should align with the specific needs of your practice. Systems with high accuracy, such as those using confocal microscopy (e.g., TRIOS) or advanced structured light (e.g., Primescan), are ideal for full-arch work. On the other hand, scanners with moderate accuracy are sufficient for simpler tasks like single crowns or short-span bridges [3][13][7]. The way you scan also matters – a linear or combined scanning pattern tends to produce better trueness and precision compared to zig-zag patterns [5]. As researcher Florian Kernen explains:
"The accuracy of intraoral scanners is a prerequisite for the fabrication of dental restorations in computer-aided design and computer-aided manufacturing (CAD-CAM) dentistry" [1].
However, performance can vary due to practical challenges. Factors like the size of the scanner head, operator skill, and intraoral conditions (e.g., saliva) often lead to results that differ from controlled laboratory settings [1][2][7][14].
Digital workflows offer time-saving benefits, cutting about 8.6 minutes per procedure. This not only boosts productivity but also improves patient comfort. That said, it’s worth noting that stereolithography printers can add approximately 49 ± 9 μm of error to the overall process [3][13]. Keep in mind, though, that the ultimate accuracy of restorations hinges on the entire digital workflow.
When investing in a scanner, Australian dentists should prioritise systems with open architecture and file formats like PLY or OBJ, which facilitate smoother collaboration with dental labs. Additionally, ensure compatibility with specific treatment systems – some cases, such as Invisalign, may require particular scanners [14]. These considerations highlight the importance of further research into how scanners perform under real-world conditions.
Study Limitations and Areas for Further Research
This study offers useful benchmarks for scanner performance, but its laboratory-based approach comes with limitations. The research relied on rigid models, such as PEEK or stone, which don’t mimic the complexities of scanning live patients. As Mattia Sacher from the University of Basel points out:
"This experimental study avoided the presence of soft tissues, saliva, blood, filling materials, or space limitations, which often can compromise the accuracy of the scan data in a clinical setting" [13].
In clinical practice, scanning is far more challenging. Variables like saliva, moisture, and lens wetting can obscure the scan field, while physical constraints – limited mouth opening, tongue movement, or the gag reflex – further complicate the process. Additionally, real teeth exhibit mobility (ranging from 30 to 100 μm in live patients), a factor absent when using rigid models [13]. These real-world conditions significantly impact scan accuracy, with the median trueness of long-span intraoral scans in clinical settings measured at 433 μm, much higher than the deviations observed in laboratory conditions [1].
Another limitation is the study’s small sample size, which restricts the ability to generalise findings. Many studies on scanner accuracy involve small cohorts, typically between 5 and 30 participants, limiting their statistical reliability [11]. Furthermore, these studies often rely on a single experienced operator, which could inflate accuracy results compared to those achieved by less experienced practitioners or recent graduates. L. Lanteri from UniCamillus University highlights:
"The limitations of this study are the small size of the sample and its cross-sectional nature. Future studies should include a larger sample to validate the findings and ensure they are generalizable" [11].
Examiner variability also poses a challenge, with diagnostic sensitivity differing by as much as 32% between individuals, further emphasising the need for standardised training and calibration protocols [12].
To address these gaps, future research should focus on in vivo studies conducted in diverse Australian clinical settings. These studies should consider patient demographics, complex dental conditions (like edentulous arches, paediatric cases, and enamel defects), and varying levels of practitioner expertise. Multi-centre research with larger cohorts would be essential to determine whether the results observed in controlled environments hold true in everyday practice, both in metropolitan and regional areas across Australia.
Conclusion
The accuracy of dental scanners varies depending on the application. For full-arch and complex implant cases, the TRIOS 3 and Primescan consistently deliver top-tier performance. For example, the TRIOS 3 achieves a trueness of 38 μm for maxillary all-on-four implants [7]. However, accuracy tends to decrease with longer scans, with long-span scans reaching up to 433 μm – well above the acceptable 100 μm threshold for a proper fit [1][6].
These differences in performance have a direct impact on clinical workflows, especially in Australian practices. Digital impressions, for instance, save an average of 8.59 minutes per procedure compared to traditional methods [3]. This is particularly relevant in Australia, where nearly 30% of patients delay or avoid dental care due to costs [15]. Choosing the right scanner for specific case types – whether for single crowns, quadrant work, or full-arch prosthetics – can significantly affect restoration accuracy, minimise chairside adjustments, and enhance patient comfort.
The study also underscores the importance of operator expertise and clinical conditions. Experienced TRIOS 3 users achieved RMS values of 0.057 mm, nearly three times better than results from students [2]. Real-world challenges like saliva, moisture, and limited access can also influence scanning accuracy.
Ultimately, success depends on selecting the right scanner for the clinical situation and ensuring proper training. Australian dentists should consider their practice’s needs, invest in structured training programs, and opt for high-end scanners for complex cases. This approach ensures predictable, high-quality restorations while maintaining efficiency and improving patient care.
FAQs
Why are trueness and precision important when choosing an intraoral scanner?
When choosing an intraoral scanner, trueness and precision are two key aspects to look for, as they directly impact the accuracy of digital impressions. Trueness measures how closely the scan reflects the actual shape and structure of the teeth, while precision focuses on the scanner’s ability to deliver consistent and repeatable results.
Scanners with strong performance in both areas are crucial for creating accurate digital models, which play a vital role in treatments like dental implants, crowns, and orthodontics. Research has pointed to devices such as the CEREC Primescan and Trios 3 as being among the most dependable options, offering reliable results that contribute to improved patient outcomes.
Why are full-arch scans generally less accurate than shorter scans?
When performing full-arch scans, a larger section of the mouth is captured. This process involves more image stitching and takes longer, which can sometimes result in minor errors building up across the arch. These errors can affect trueness (how accurately the scan reflects the actual shape) and precision (how consistently the scan can replicate results). On the other hand, shorter scans target smaller areas, often achieving higher accuracy with fewer chances for errors.
What should Australian dentists look for when choosing an intraoral scanner?
When choosing an intraoral scanner (IOS), Australian dentists should focus on accuracy, which encompasses both trueness – how well the scan represents the actual anatomy – and precision, or the consistency of results across multiple scans. It’s worth noting that full-arch scans tend to show greater deviations compared to smaller areas, making it crucial to select a scanner that minimises errors across the entire arch. Factors like the number of alignment points captured during the scan also play a role in achieving accurate results.
Efficiency and patient comfort should also be high on the priority list. Scanners that offer faster capture times and seamless data acquisition can significantly improve workflow efficiency while providing a more comfortable experience for patients compared to traditional impression methods. Additionally, ensuring the scanner is compatible with your practice’s CAD/CAM system can simplify post-scan processing and make treatment planning more straightforward.
Lastly, think about operator expertise and how well the scanner suits specific clinical needs, whether it’s for orthodontics, implants, or restorative work. Access to training and ongoing support is vital to make the most of the scanner’s capabilities. This not only ensures reliable outcomes but also supports compliance with Australian dental standards.
Related Blog Posts
- Intraoral Scanners vs. Impressions: Accuracy Compared
- How Intraoral Scanners Improve Orthodontic Workflows
- Future of Intraoral Scanners in Orthodontics
- Recent Advances in Intraoral Scanning Technology
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





