







Studies on Laser Gum Surgery Patient Selection

Laser gum surgery, especially using protocols like LANAP (Laser-Assisted New Attachment Procedure), is highly effective for treating advanced gum disease. However, not everyone is a suitable candidate. Here’s what you need to know:
- Best Candidates: Patients with deep periodontal pockets (≥7 mm) benefit most. Accurate periodontal pocket depth measurement is essential for determining these candidates. Lasers can target bacteria and promote tissue regeneration where traditional methods fall short.
- Moderate Cases: For pockets between 4–6 mm, the advantages of laser treatments over scaling and root planing (SRP) are limited.
- Systemic Health: Conditions like diabetes or cardiovascular issues may influence outcomes. Smoking and poor oral hygiene reduce success rates significantly.
- Procedure Benefits: Laser treatments often result in less post-operative pain and faster healing compared to conventional methods.
- Key Risks: Incorrect laser settings or poor technique can cause thermal damage. Smoking and uncontrolled systemic conditions also increase risks.
This article reviews the clinical criteria, research findings, and practical considerations for laser gum surgery in Australia, helping dentists and patients make informed decisions.
Core Clinical Criteria for Patient Selection
Periodontal Disease Severity and Treatment Indications
When deciding if laser-assisted periodontal surgery is the right choice, pocket depth is the main clinical factor to consider. This approach is particularly beneficial for periodontal pockets measuring 7 mm or more, as conventional scaling and root planing (SRP) often struggle to completely eradicate harmful bacteria in these cases [2].
For moderate pockets (4–6 mm), the benefits of laser therapy are less pronounced. Some studies report small improvements in clinical attachment levels (CAL), while others find no meaningful difference compared to SRP alone [2][7]. For example:
"LLLT with the chosen settings did not show a beneficial effect during the initial nonsurgical treatment of periodontitis." [7]
When it comes to intra-bony defects, laser therapy is typically recommended for probing depths of 5 mm or more, paired with defect depths of at least 3 mm. This method can aid early wound healing and encourage bone regeneration [4]. Additionally, Low-Level Laser Therapy (LLLT) may help reduce gingival recession during the healing process [2].
| Pocket Severity | Probing Depth | Suitability for Laser Surgery | Key Outcome |
|---|---|---|---|
| Moderate | 4–6 mm | Low to moderate | Minor CAL gain; control of recession [2] |
| Deep | ≥7 mm | High | Reduction in pocket depth; CAL gain [2] |
| Intra-bony Defects | ≥5 mm (≥3 mm defect) | Moderate | Early wound healing; bone regeneration [4] |
While pocket depth is a critical measure, systemic health and other patient factors also play a role in determining suitability.
Systemic Health Factors
Although pocket depth is the primary criterion, a patient’s overall health can significantly influence the decision to proceed with laser gum surgery. Since these procedures generally require only local anaesthesia, they are often a safer option for patients at higher risk from general anaesthesia, such as those with cardiovascular issues [8].
For individuals with Type 2 diabetes, studies suggest that diode laser therapy can enhance periodontal outcomes [10]. Laser therapy also offers an alternative for patients with a history of antibiotic sensitivity or resistance. By reducing bacterial loads – such as Porphyromonas gingivalis – it avoids the systemic side effects and resistance issues linked to long-term antibiotic use [9]:
"Laser therapy can be considered as an effective treatment modality in stage III grade C periodontitis, avoiding the systemic antibiotic side effects and solving the recurrence problems due to bacterial resistance by long term usage." – BMC Oral Health [9]
Pregnancy complicates patient selection, as most clinical trials exclude pregnant and breastfeeding individuals to prioritise safety [9]. Meanwhile, smoking presents another obstacle. Many studies exclude smokers or require them to abstain during the healing process, as smoking severely impairs tissue repair and compromises treatment outcomes [8][9].
Oral Hygiene and Patient Behaviour
Beyond clinical and systemic factors, oral hygiene and patient commitment are crucial for successful outcomes. Laser-assisted surgery demands excellent oral care. Most clinical trials include only those patients who have already undergone Phase I therapy (scaling and root planing) and demonstrated consistent self-care [1][4]. In clinical practice, patients with residual pockets of 5 mm or more and intra-bony defects of 3 mm or more are typically considered for laser treatment only after establishing a proper hygiene routine [4].
The early healing phase is especially sensitive:
"The stability of the wound surface during the early healing stage depends on the suturing effect, but it is crucial to ensure that it is not compromised by plaque re‐colonisation." [4]
After surgery, patients are advised to avoid brushing or flossing the treated area for about a week. Instead, gentle rinsing with warm salt water is recommended, avoiding forceful spitting. These precautions help protect the fibrin clot formed by the laser. Without regular professional maintenance and diligent home care, even the modest 0.34 mm additional pocket depth reduction achieved by LLLT at three months [4] can be lost.
sbb-itb-2be92ed
LANAP Procedure Step-by-Step. Laser Gum Treatment with Dr. Sandak. Live Patient Demonstration.
Laser Surgery Versus Conventional Periodontal Treatments
Laser vs Conventional Gum Surgery: Patient Selection & Clinical Outcomes
Where Laser and Conventional Treatments Overlap or Differ
Both laser-assisted and conventional surgeries aim to achieve similar goals: reducing pocket depths, removing diseased tissue, and encouraging tissue reattachment. In many cases, lasers are used alongside conventional techniques, such as the Kirkland flap, rather than as a complete replacement. This combination approach helps tailor treatments to specific patient needs.
However, the two methods differ in how they address certain clinical situations. For deep periodontal pockets (≥ 7 mm), cases unresponsive to Phase I therapy, or instances where minimising gingival recession is crucial, flapless laser-assisted treatments have shown clear advantages over traditional debridement alone [2][12]. On the other hand, for moderate periodontitis managed with standard scaling and root planing, current research does not support routinely adding lasers to non-surgical treatments [7]. These distinctions set the stage for comparing the clinical outcomes of each approach.
What the Evidence Shows on Clinical Outcomes
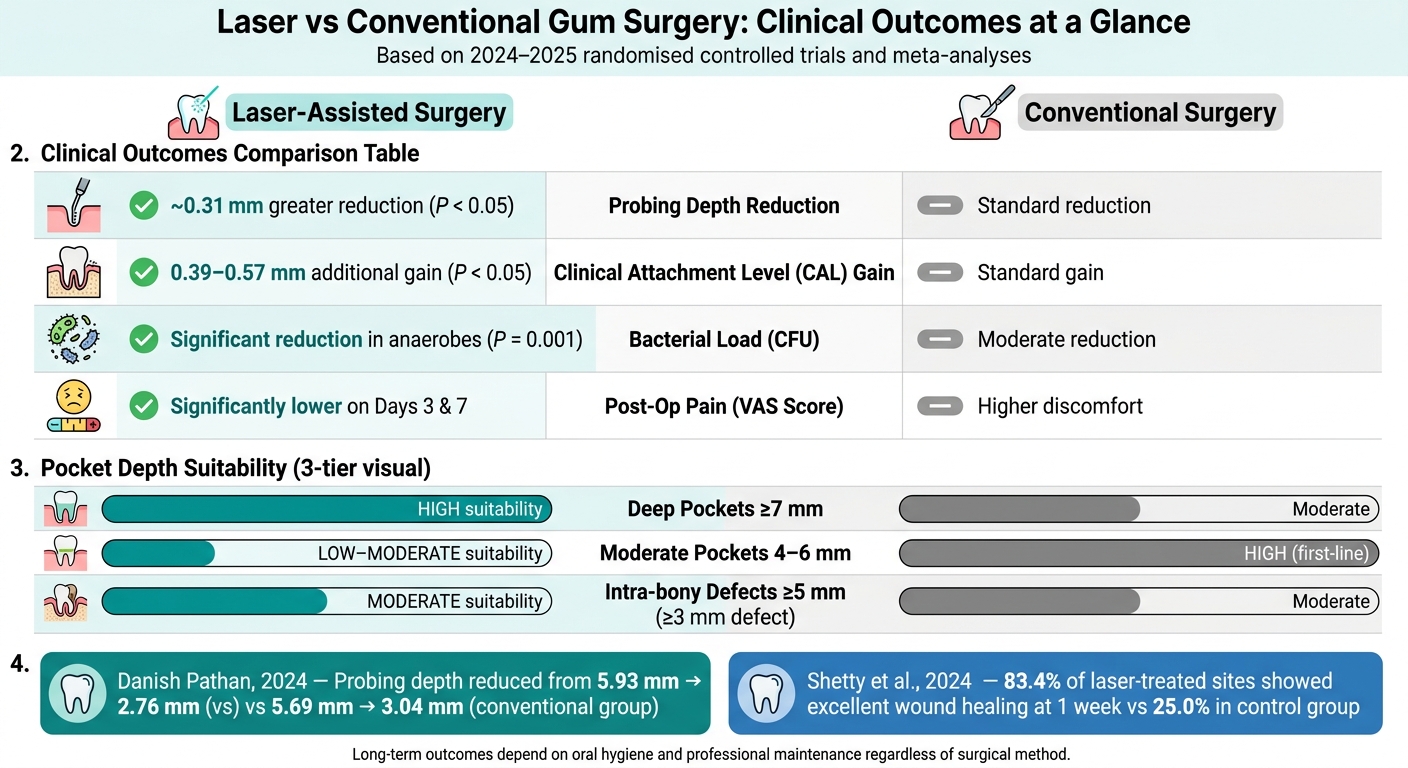
Clinical studies tend to favour laser-assisted surgery, particularly in the short-to-medium term. A 2025 meta-analysis of 12 randomised controlled trials revealed that laser-assisted open flap debridement led to a mean additional probing depth reduction of 0.31 mm and a mean additional clinical attachment level (CAL) gain of 0.57 mm compared to conventional open flap debridement at six months [11]. Supporting this, a February 2024 study by Danish Pathan reported that probing depths in the laser group decreased from 5.93 mm to 2.76 mm, compared to 5.69 mm to 3.04 mm in the conventional group. Additionally, the laser group showed a significantly greater reduction in colony-forming units (CFU) of obligate anaerobes [12]:
"The application of ND:YAG laser as an adjunctive tool to open flap debridement have demonstrated a better outcome in management of persistent deep periodontal pockets in terms of probing depth reduction and greater reduction in CFU of obligate anaerobes." – Danish Pathan et al. [12]
Interestingly, while laser-assisted surgery initially outperforms conventional methods, the gap in outcomes narrows between six and twelve months. Long-term success often depends more on good oral hygiene and regular professional maintenance than on the surgical method itself.
| Clinical Parameter | Laser-Assisted (Adjunctive) | Conventional Surgery | Significance |
|---|---|---|---|
| Probing Depth (PD) | ~0.31 mm greater reduction [11] | Standard reduction | Significant (P < 0.05) |
| Clinical Attachment (CAL) | ~0.39–0.57 mm additional gain [11][4] | Standard gain | Significant (P < 0.05) |
| Bacterial Load (CFU) | Significant reduction in anaerobes [12] | Moderate reduction | Significant (P = 0.001) |
| Gingival Recession | No significant difference [2] | No significant difference | Non-significant |
Benefits and Limitations of Laser-Assisted Surgery
One key advantage of laser-assisted surgery is reduced post-operative discomfort. A February 2024 split-mouth randomised clinical trial by Dr. Vineet V. at Sri Ramachandra Dental College demonstrated that using a 445 nm diode laser (0.8 W, continuous wave mode) as an adjunct to Kirkland flap surgery significantly lowered Visual Analog Scale (VAS) pain scores on days 3 and 7 compared to conventional surgery alone [1]:
"Adjunctive use of laser (445 nm wavelength) can be recommended for achieving more predictable clinical outcomes. VAS score indicative of post-surgical discomfort were also lower for the laser treated sites." – Vineet V. et al. [1]
The science behind this lies in photobiomodulation. Laser energy enhances ATP production, promotes angiogenesis, and reduces inflammatory mediators, speeding up soft tissue healing.
That said, laser-assisted surgery has its challenges. Success heavily depends on the clinician’s expertise in adjusting laser parameters like wavelength, power output, pulse mode, and exposure duration. Poor technique can diminish results or, worse, cause thermal damage to surrounding tissues. Strict adherence to safety protocols – such as controlled sweeping motions and pauses during continuous irradiation – is critical [6]. Additionally, the lack of standardised laser settings across clinical trials highlights the need for consistency to ensure reliable and comparable results.
Outcomes and Risks by Patient Profile
Clinical and Patient-Reported Outcomes Across Patient Groups
Patient outcomes differ significantly depending on the depth of periodontal pockets. Deep pockets (≥ 7 mm) tend to show the most improvement, while moderate pockets (4–6 mm) respond similarly to traditional treatments [2]. These findings align with earlier insights into how disease severity, systemic health, and oral hygiene influence outcomes.
A May 2023 randomised controlled trial led by Jia-wei Lu at Tongji University studied 67 mandibular second molars with 154 residual pockets. The trial compared the effects of an 810 nm diode laser (1.5 W, up to 40 seconds) used alongside non-surgical therapy to conventional treatment. At the 24-week mark, the laser group achieved a mean probing pocket depth of 3.06 mm, compared to 4.46 mm in the conventional group. Bleeding on probing also reduced significantly – 15.49% in laser-treated sites versus 64.29% in those treated conventionally [5]:
"Diode laser as an adjunct to nonsurgical periodontal therapy may contribute to the clinical outcomes for residual periodontal pockets in mandibular second molars." – Li-jun Luo, Stomatological Hospital and Dental School of Tongji University [5]
Patient feedback supports these clinical findings. In October 2024, a study led by Dr. Bhavya Shetty at Ramaiah University of Applied Sciences in Bangalore investigated photobiomodulation using a 1064 nm diode laser after flap surgery in 24 patients with 5–8 mm deep pockets. The results were striking: 83.4% of laser-treated sites showed excellent wound healing within one week, compared to just 25.0% in the control group. Additionally, pain scores on the Wong-Baker FACES scale were significantly lower for the laser group [13]:
"Patients’ reported pain and painkiller usage dramatically decreased following flap surgery using the 1064-nm diode laser." – Shetty et al., Ramaiah University of Applied Sciences [13]
While these results are promising, they also highlight the importance of understanding associated risks.
Safety Concerns and Contraindications
High-power laser treatments carry the potential risk of thermal injury to the gingiva and bone. To mitigate this, clinicians typically employ physiological saline irrigation and adhere to standardised power settings – usually between 3.0 W and 4.0 W, depending on the stage of the procedure [2]. However, particular caution is advised when using 810 nm diode lasers near mandibular molars, as they may reduce the width of keratinised tissue, requiring close monitoring [5].
Certain patient groups are routinely excluded from research due to safety concerns or the potential for compromised outcomes. Smokers are often excluded because of their impaired wound-healing capacity. Similarly, pregnant or lactating women are excluded, as safety data for these groups is lacking in clinical trials. Patients with uncontrolled systemic conditions – such as diabetes, hypertension, coronary heart disease, or atherosclerosis – face a higher risk of reduced long-term stability following laser procedures [4][2].
| Patient Profile | Risk or Consideration | Research Status |
|---|---|---|
| Smokers | Impaired healing; excluded from efficacy trials | High risk [4][2] |
| Uncontrolled diabetes / heart disease | Reduced long-term attachment stability | High risk [4] |
| Pregnancy / lactation | Safety not established in clinical trials | Excluded [4][2] |
| Patients prone to recession | LLLT may reduce post-operative recession severity | Lower risk [2] |
Understanding these risks is crucial for ensuring patient safety and optimising outcomes.
Long-Term Stability and Maintenance
Achieving long-term stability depends heavily on patient adherence to oral hygiene routines and participation in structured maintenance programmes. Without consistent care, the benefits of laser treatments can diminish over time [4][2].
Researchers have also highlighted the lack of standardised treatment protocols across studies, which complicates drawing definitive conclusions about long-term outcomes. Moving forward, combining laser therapy with regular maintenance and addressing systemic health conditions before and after treatment will likely provide patients with the best chance for lasting success [7][2].
Applying Research Findings in Australian Clinical Practice
Selecting Patients Based on Evidence
Australian clinicians, operating under AHPRA and Dental Board of Australia guidelines, can use the latest evidence to fine-tune patient selection for laser-assisted periodontal surgery. Research indicates that for periodontal pockets measuring ≥7 mm, adjunctive laser therapy surpasses scaling and root planing (SRP) alone in reducing pocket depth and improving clinical attachment levels [2][6]. For moderate pockets (4–6 mm), conventional SRP remains a reliable first-line treatment.
When choosing a laser modality, intensity plays a crucial role. High-intensity diode laser therapy (DLT-H), used at approximately 2.0 W, has shown a clinical attachment level (CAL) gain of 2.20 ± 0.45 mm at three months – a notable improvement over the 1.72 ± 0.51 mm gain achieved with SRP alone [6]. In contrast, low-intensity settings primarily aid in tissue repair and early wound healing rather than contributing to significant attachment gain. These findings are pivotal for tailoring treatment plans and communicating options effectively to patients.
"Integrating high-intensity diode laser therapy as an adjunct to nonsurgical periodontitis management provides significant short-term clinical benefits, particularly in CAL improvement and inflammation control." – Nature Scientific Reports [6]
Informed Consent and Patient Education
Clear and open communication is a cornerstone of patient care under AHPRA guidelines. Patients need to be informed that laser therapy is an adjunct to conventional treatment, and long-term outcomes depend heavily on consistent oral hygiene and regular professional care [4][2]. It’s essential to set realistic expectations: while lasers can reduce discomfort and enhance early healing, they don’t significantly impact plaque control compared to traditional cleaning methods [3][6]. Additionally, the lack of a unified protocol for adjunctive laser therapy in periodontitis should be discussed to ensure transparency [7].
Treatment Planning That Combines Laser and Conventional Approaches
Combining laser technology with conventional methods can maximise outcomes, especially for non-surgical cases involving deep pockets. High-intensity diode lasers are particularly effective for decontamination and epithelial debridement in areas where mechanical tools have limited access. For surgical flap procedures, using a 445 nm diode laser in non-contact mode (0.8 W, continuous wave) has been shown to lower post-operative pain and improve short-term results [1].
"The adjunctive use of 445 nm diode laser to surgical periodontal therapy contributed to improved short-term clinical outcomes… VAS scores indicative of post-surgical discomfort were also lower for the laser-treated sites." – Lasers in Medical Science [1]
For regenerative treatments, especially those involving intra-bony defects, the Laser-Assisted New Attachment Procedure (LANAP) with an Nd:YAG laser supports bone regeneration and new attachment formation in deep pockets [2]. During the healing phase, low-level laser therapy (LLLT) at approximately 0.5 W in non-contact mode can assist in reducing recession risk and promoting cellular repair [6].
| Laser Modality | Recommended Setting | Best-Suited Application |
|---|---|---|
| High-intensity diode (DLT-H) | 2.0 W, contact mode | Deep pockets ≥ 7 mm; decontamination and CAL gain [6] |
| Low-level laser (LLLT/DLT-L) | 0.5 W, non-contact mode | Post-operative healing; recession-prone sites [6] |
| 445 nm diode | 0.8 W, non-contact mode | Adjunct to flap surgery; pain reduction [1] |
| Nd:YAG (LANAP) | Pulsed mode | Regenerative cases; bone filling in deep pockets [2] |
This blended approach complies with Australian standards and AHPRA guidelines, ensuring treatments are both evidence-based and patient-centred.
Key Takeaways on Patient Selection for Laser Gum Surgery
Laser-assisted periodontal surgery isn’t suitable for every gum disease patient. Research highlights its effectiveness for patients with deep residual pockets (≥7 mm), where traditional scaling and root planing often fall short [2][6]. For patients with moderate pocket depths (4–6 mm), standard mechanical debridement remains the go-to treatment approach.
Patient selection relies on specific clinical criteria. Candidates are typically identified by factors like probing depths, attachment loss, and radiographic evidence of bone loss that meet established benchmarks [4][7][2]. Additionally, non-smokers are preferred due to the well-known negative impact of smoking on periodontal healing. After completing initial periodontal therapy, patients must also demonstrate consistent oral hygiene practices. This ensures that the laser treatment works as intended, rather than compensating for inadequate home care [4][2].
The laser type should align with the treatment goal. LANAP (Nd:YAG) is ideal for achieving periodontal regeneration [2]. High-intensity diode lasers are effective for decontamination and improving attachment in deep pockets, while low-level laser therapy (LLLT) is better suited for enhancing early wound healing and reducing the risk of gum recession during recovery [2][6]. By incorporating these criteria, clinicians can create tailored treatment plans grounded in current research.
With around 42% of adults over 35 experiencing moderate periodontitis and 10% facing severe forms [7], there is a significant pool of potential candidates. Applying these selection guidelines helps ensure better outcomes through careful and personalised screening.
FAQs
How do I know if my gum pockets are deep enough for laser treatment?
Gum pockets are typically deemed suitable for laser treatment when their probing depth reaches 4 mm or more. This level of depth is often linked to periodontal disease, making laser-assisted therapy a potential option. It’s crucial to consult your dentist to evaluate your condition and determine the most appropriate treatment for your needs.
What medical conditions can make laser gum surgery less suitable?
Certain health conditions, like advanced gum disease, systemic illnesses, or specific oral health complications, might limit the suitability of laser gum surgery. These issues can affect the healing process and influence the treatment’s outcome.
What aftercare is needed to keep laser gum surgery results long-term?
To keep your gums healthy after laser gum surgery, focus on maintaining strong oral hygiene habits. Brush and floss daily, and don’t skip your regular professional cleanings. It’s also important to keep an eye on your gum health to catch any signs of gum disease early. Staying consistent with these practices is essential for protecting your results and ensuring your overall oral health stays on track.
Related Blog Posts
- Advances in Periodontal Antimicrobial Therapy
- Laser vs. Traditional Gum Surgery
- Diode vs. Erbium Lasers: Periodontal Tissue Effects
- 5 Benefits of Soft Tissue Laser Dentistry
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





