







Periodontal vs. Endodontic Lesions: Key Differences
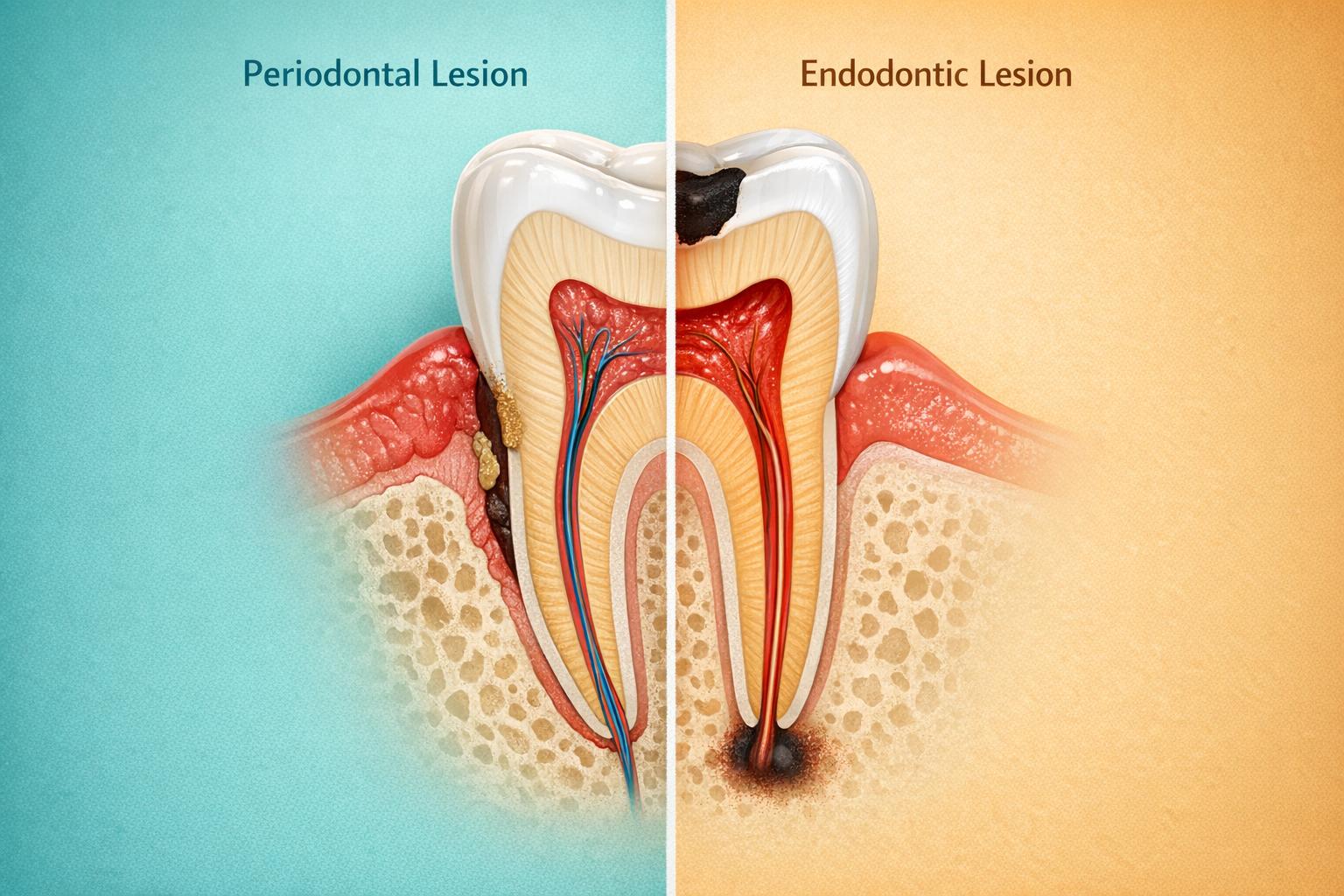
When your tooth hurts or shows swelling, the cause might be harder to pinpoint than you think. Two common dental issues – periodontal lesions and endodontic lesions – are often confused. They may look alike, but they come from completely different origins and need different treatments.
Here’s the key difference:
- Periodontal lesions start at the gumline and progress downward, usually caused by plaque and calculus build-up.
- Endodontic lesions begin inside the tooth when the pulp gets infected or dies, spreading outward to surrounding tissues.
Getting the diagnosis right is critical because treating the wrong issue won’t fix the problem. For example, scaling won’t help an infected pulp, and a root canal won’t solve early signs of gum disease.
Quick Comparison
| Feature | Periodontal Lesion | Endodontic Lesion |
|---|---|---|
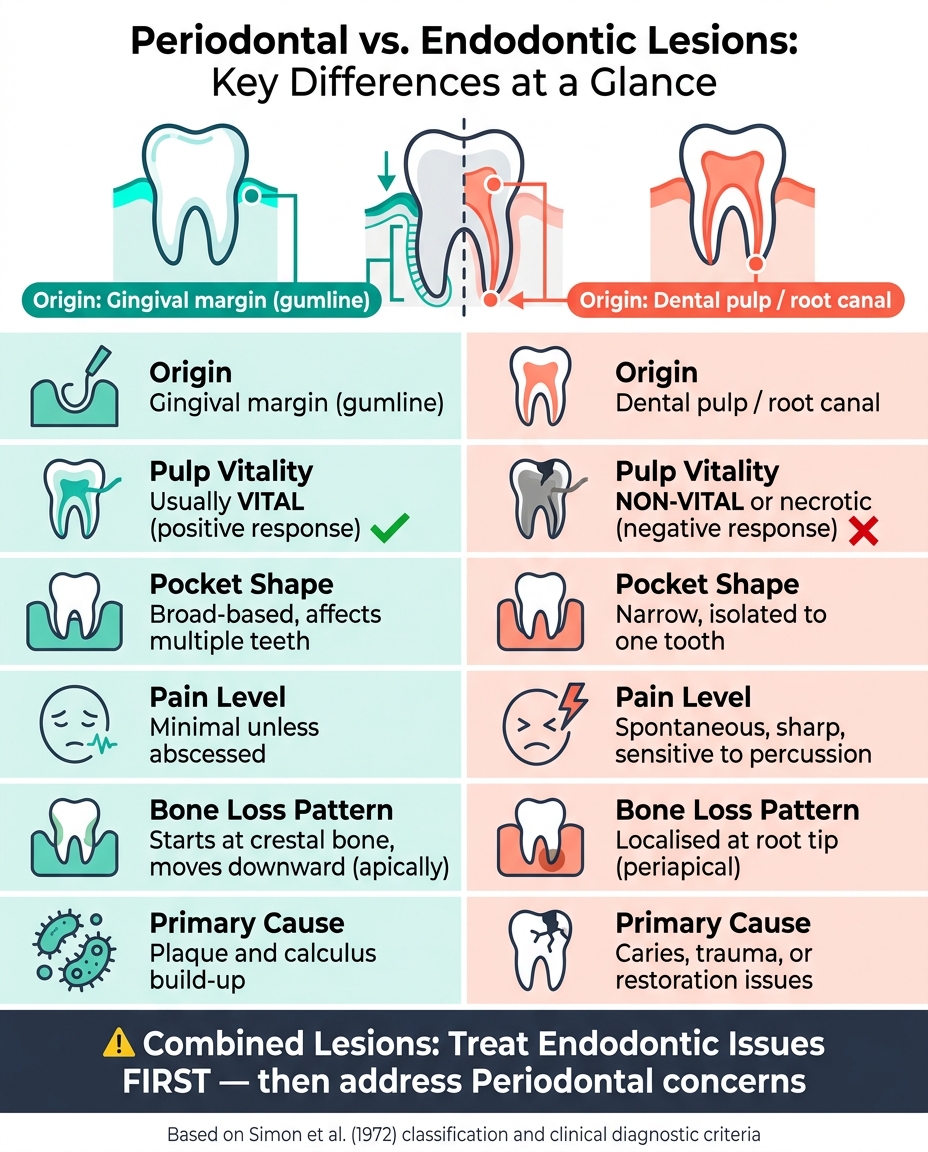
| Origin | Gingival margin | Dental pulp/root canal |
| Pulp Vitality | Usually vital | Non-vital or necrotic |
| Pocket Shape | Broad-based, affects multiple teeth | Narrow, isolated to one tooth |
| Pain | Minimal unless abscessed | Sharp, spontaneous, sensitive to touch |
| Bone Loss Pattern | Starts at crestal bone, moves downward | Localised at root tip |
In cases where both conditions overlap (combined lesions), endodontic therapy should come first to address the internal infection, followed by periodontal treatment if needed. Early and accurate diagnosis is key to saving the tooth and preventing unnecessary procedures.
Periodontal vs. Endodontic Lesions: Key Differences at a Glance
Causes and Disease Pathways
Causes of Periodontal Lesions
Periodontal lesions begin with the build-up of bacterial biofilm along the gumline. Over time, this biofilm hardens into calculus, triggering chronic inflammation. This inflammation progressively damages the gum tissue, periodontal ligament, and alveolar bone [2].
Both systemic and local factors can speed up this process. Conditions like poorly controlled diabetes, smoking, and chronic stress weaken the body’s ability to fight off infection. Meanwhile, anatomical features such as furcation involvement or palato-gingival grooves create areas where plaque is hard to remove, allowing it to accumulate unchecked [1][2].
Causes of Endodontic Lesions
Endodontic lesions originate from damage within the tooth. Deep decay, trauma, or cracks can allow bacteria to penetrate the enamel and dentine, eventually infecting the pulp. This infection, known as pulpitis, can progress to pulpal necrosis if untreated [1][2].
Once the pulp is infected, bacteria and their by-products can escape through the root canal system. As Evans from the University of Melbourne explains:
"The apical foramen is arguably the principal route of communication between the pulp and periodontal tissues, mainly due to its size relative to the other anatomical pathways." [2]
Additional routes, such as lateral and accessory canals, especially in the apical third of the root, can also facilitate the spread of infection [1]. Iatrogenic issues like root perforations or poor coronal seals may further contribute to the development of endodontic lesions [1]. Unlike periodontal lesions, these infections originate inside the tooth, presenting unique clinical challenges.
Combined Endo-Perio Lesions
When periodontal and endodontic infections overlap, diagnosing and managing the condition becomes more complicated. These combined endo-perio lesions (EPLs) can arise independently or one condition may directly influence the other.
The classification by Simon et al. (1972) is widely used to categorise these lesions based on their origin:
| Classification | How It Develops |
|---|---|
| Primary Endodontic | Pulp necrosis leads to apical periodontitis, which may drain through the periodontal ligament, creating a pocket-like appearance. |
| Primary Endo with Secondary Periodontal | An untreated endodontic infection forms a drainage tract, where plaque and calculus build up over time. |
| Primary Periodontal | Disease progresses downward from the gumline while the pulp remains healthy initially. |
| Primary Perio with Secondary Endodontic | A deep periodontal pocket eventually reaches the apical foramen or a lateral canal, causing pulp necrosis. |
| True Combined Lesion | Separate endodontic and periodontal lesions develop independently but eventually merge along the root. |
These combined lesions are further complicated by overlapping microbiology. Bacteria commonly linked to periodontal disease – such as Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola – are often found in infected root canals as well [1]. This microbial similarity makes it difficult to determine which condition appeared first, complicating both diagnosis and treatment planning. These challenges pave the way for the detailed treatment strategies discussed in the following sections.
sbb-itb-2be92ed
Clinical Signs, Symptoms, and Diagnostic Tools
Signs and Symptoms of Periodontal Lesions
Periodontal lesions often creep in quietly, developing over time without causing immediate alarm. Common signs include bleeding gums, bad breath, gum recession, and loose teeth. Pain is usually absent unless an acute abscess forms. During an examination, periodontal probing typically uncovers broad-based pockets that span across multiple teeth. These pockets are often accompanied by visible plaque and calculus deposits. On X-rays, the bone loss usually starts at the crestal bone and progresses either horizontally or in an angular pattern, often affecting multiple teeth rather than just one.
Signs and Symptoms of Endodontic Lesions
Endodontic lesions tend to make their presence known more dramatically. Patients often report spontaneous pain, sensitivity to temperature changes, and discomfort when biting. There may also be a draining sinus tract near the gumline. A non-vital pulp test – where the tooth fails to respond to pulp sensibility testing – strongly points to an endodontic origin. On radiographs, these lesions are frequently marked by a periapical radiolucency – a dark shadow near the root tip – indicating localised bone resorption caused by an infection originating within the tooth.
How to Tell the Two Lesions Apart
Differentiating between periodontal and endodontic lesions hinges on combining clinical observations with specific diagnostic tests. Among these, pulp sensibility testing is the most critical. A tooth that responds positively to cold (CO₂) or electric pulp testing suggests a periodontal issue, while a lack of response typically indicates pulpal necrosis and an endodontic cause.
The shape and location of the periodontal pocket can also provide valuable insights. Periodontal pockets are generally broad and affect multiple teeth, whereas an endodontic infection draining through the periodontal ligament often creates a narrow, isolated pocket on a single tooth. The direction of disease progression further distinguishes the two: periodontal disease spreads downward from the gumline, while endodontic infections move upward from the tooth’s apex – a phenomenon known as retrograde periodontitis.
Here’s a quick comparison of the two:
| Feature | Periodontal Lesion | Endodontic Lesion |
|---|---|---|
| Pulp Vitality | Vital (positive response) | Non-vital (negative response) |
| Pocket Shape | Broad-based, involving multiple teeth | Narrow, isolated to one tooth |
| Pain | Minimal unless abscessed | Spontaneous, sharp, and sensitive to percussion |
| Bone Loss Pattern | Starts at the crestal bone, moves apically | Localised at the root tip or surrounding area |
| Calculus/Plaque | Commonly present | Often absent |
| Tooth Mobility | Generalised and progressive | Localised, may improve after treatment |
For more challenging cases, advanced imaging such as Cone-Beam Computed Tomography (CBCT) can be a game-changer. CBCT helps identify root fractures, perforations, or resorption that standard 2D radiographs might miss. It’s also helpful when the rest of the mouth appears healthy, but a single tooth shows a deep pocket, especially if it has a large restoration or a history of trauma. In such cases, an endodontic origin is highly likely.
Treatment: Periodontal vs. Endodontic Lesions
Treating Periodontal Lesions
The treatment for periodontal lesions focuses on managing the underlying causes, such as poor oral hygiene, smoking, or diabetes. The primary method is scaling and root planing (SRP), which targets plaque and calculus buildup responsible for inflammation and bone loss.
If SRP doesn’t resolve deeper defects, periodontal surgery may be required to clean areas that cannot be reached non-surgically. Long-term success hinges on consistent professional cleanings and good oral hygiene at home.
Endodontic lesions, however, require a different approach, as their source lies within the tooth.
Treating Endodontic Lesions
Endodontic treatment revolves around root canal therapy. This involves removing the infected pulp, disinfecting the canals, and sealing them to prevent reinfection. Between appointments, intracanal calcium hydroxide is often used to reduce bacteria.
If the initial root canal fails, options like retreatment or an apicoectomy (removal of the root tip) may be explored. Endodontic lesions generally have a positive outlook – once the infection is eliminated, the surrounding bone often heals effectively.
When both periodontal and endodontic issues occur together, a carefully planned approach is essential.
Managing Combined Endo-Perio Lesions
Treating combined lesions requires a step-by-step strategy. Since the origins differ, the endodontic therapy must come first. This eliminates the internal infection, allowing the periodontal tissues time to heal and revealing the true extent of the periodontal defect.
While scaling and root planing (SRP) can be done alongside root canal therapy, surgical interventions should wait. A monitoring phase – lasting anywhere from a few weeks to six months – helps assess tissue response. As M. Evans from the University of Melbourne explains:
"It is often only after this monitoring phase that the extent of the endodontic contribution can be fully assessed. This, in turn, allows for a more accurate assessment of the periodontal condition and periodontal treatment needs." [2]
The outlook for combined lesions is less certain, especially for single-rooted teeth with deep defects that connect to the apex. For multi-rooted teeth, procedures like root resection or hemisection may be options if enough support remains. Before deciding on complex treatments, high-resolution imaging, such as CBCT, is crucial to check for root fractures or perforations. These findings might shift the plan from treatment to extraction.
| Treatment Phase | Procedure | Timing |
|---|---|---|
| Phase 1 | Endodontic therapy (root canal) | First priority |
| Phase 2 | Scaling and root planing (SRP) | Concurrent with or immediately after Phase 1 |
| Phase 3 | Monitoring and re-evaluation | 1–6 months post-endodontic treatment |
| Phase 4 | Surgical periodontal therapy | If defects persist after Phase 3 |
| Phase 5 | Long-term maintenance | Ongoing |
The challenge of endo-periodontal lesions
Conclusion: Key Differences Between Periodontal and Endodontic Lesions
By looking at their causes, symptoms, and treatments, the differences between periodontal and endodontic lesions become evident. These two conditions stem from distinct origins: periodontal lesions begin at the gum margin and work their way toward the root tip, while endodontic lesions arise within the tooth’s pulp and extend outward to the surrounding tissues.
Periodontal lesions typically feature a vital pulp and broad-based pockets, whereas endodontic lesions are marked by a non-vital or necrotic pulp and narrow, isolated pockets affecting a single tooth. Diagnosing these conditions accurately relies heavily on pulp sensibility testing. In cases where root damage is suspected, advanced imaging tools like CBCT in endodontics are essential, as standard radiographs alone may not provide sufficient detail.
Here’s a quick comparison of the key differences:
| Feature | Periodontal Lesion | Endodontic Lesion |
|---|---|---|
| Origin | Gingival margin | Dental pulp / root canal |
| Progression | Toward root apex | Toward gingiva |
| Pulp Vitality | Usually vital | Non-vital or necrotic |
| Pocket Shape | Broad-based | Narrow and isolated |
| Primary Cause | Plaque and calculus | Caries, trauma, or restoration issues |
| Prognosis | Requires ongoing care | Favourable post-root canal therapy |
For cases involving combined lesions, endodontic therapy should always be performed first before addressing periodontal concerns. Treatment decisions must take into account the patient’s overall health, tooth structure, and periodontal condition. Understanding these distinctions is crucial for accurate diagnosis and effective treatment planning.
FAQs
Can gum disease cause a root canal infection?
Gum disease can indeed result in a root canal infection. This happens when advanced gum disease creates deep periodontal pockets that link to the root canal system. Through these pockets, bacteria can invade and infect the pulp tissue inside the tooth. Addressing both conditions requires accurate diagnosis and timely treatment.
How can I tell if my painful tooth is from the nerve or the gums?
Pain originating from a tooth nerve (endodontic pain) tends to be persistent and throbbing, often intensifying with exposure to hot or cold. On the other hand, pain linked to gum issues (periodontal pain) may come with swelling, bleeding, or tenderness along the gum line.
Key indicators to watch for include sensitivity to temperature changes or tapping when it’s nerve-related, while gum problems often present with deep pockets or visible inflammation. A thorough dental examination, often paired with X-rays, is typically required to pinpoint the exact cause.
Will a combined endo-perio lesion always need extraction?
A combined endo-perio lesion doesn’t automatically mean the tooth must be extracted. The treatment approach largely depends on how severe the condition is and the specific diagnosis. Often, less invasive options like root canal therapy or periodontal treatments can effectively resolve the problem. Getting an early evaluation by a dental professional is crucial to deciding the most appropriate treatment.
Related Blog Posts
- Radiographic Staging of Periodontal Diseases
- Non-Surgical vs. Surgical Periodontal Treatments: Key Differences
- Differential Diagnosis for Periodontal Infections
- Future of Endodontics: Stem Cell Therapies
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





