







Updated Guidelines for Dental Drugs in Pregnancy

Pregnancy can make oral health more challenging, and untreated dental issues may risk complications like pre-eclampsia or preterm birth. The Therapeutic Guidelines: Oral and Dental Version 4, released in late 2025, provides updated advice to ensure safe dental care during pregnancy. Key points include:
- Safe Medications: Local anaesthetics like articaine and antibiotics such as amoxicillin are safe options. For severe pain, tapentadol may be considered.
- Timing: The second trimester is ideal for non-urgent dental treatments. Emergencies, however, should be treated immediately.
- Preventive Care: Regular check-ups, good oral hygiene, and addressing dental issues before pregnancy reduce risks.
- Collaboration: Dentists should work closely with obstetricians to ensure safe care.
These guidelines aim to protect both mother and baby while addressing oral health effectively.
Safe Medications in Pregnancy (in a dental clinic) I FDA Classification
Pregnancy Drug Safety Classifications
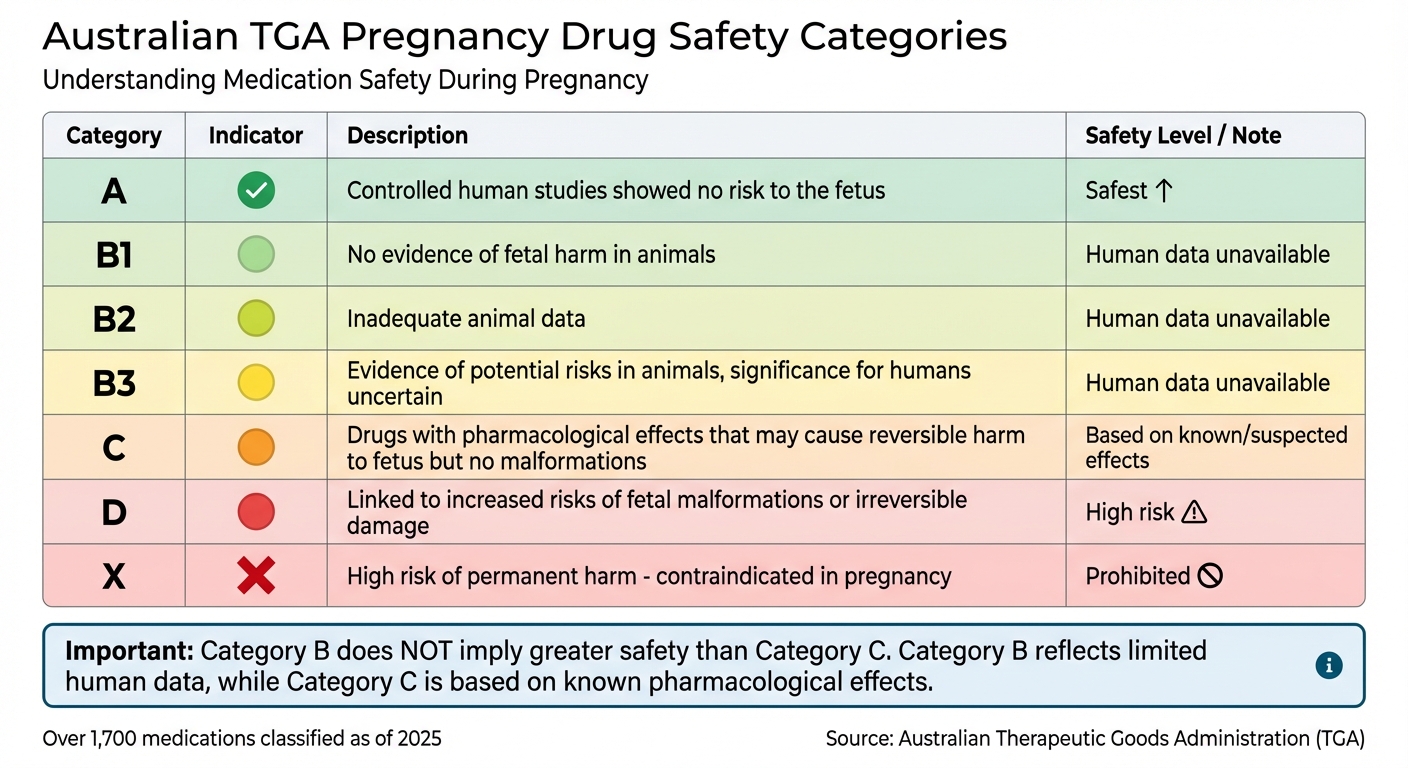
Australian TGA Pregnancy Drug Safety Categories Guide
Understanding how medications are categorised for pregnancy safety is crucial for prescribing antibiotics and managing pain in dental care. Two key systems provide guidance: the historical FDA categories and Australia’s current Therapeutic Goods Administration (TGA) classification framework.
FDA Pregnancy Categories Explained
The FDA historically used a five-letter system – A, B, C, D, and X – to classify drug safety during pregnancy. However, this system was replaced in 2015 by the Pregnancy and Lactation Labelling Rule (PLLR) [6]. Despite this update, many clinical references still mention the original categories for quick reference.
Here’s how the old FDA categories worked:
- Category A: Controlled human studies showed no risk to the foetus.
- Category B: No evidence of risk in humans, although animal studies may have shown varying results.
- Category C: Risk couldn’t be ruled out, with adverse effects seen in animal studies but insufficient human data.
- Category D: Positive evidence of risk to the human foetus, but the drug might still be used in serious situations where benefits outweigh risks.
- Category X: Contraindicated due to risks clearly outweighing any potential benefits [6].
The updated PLLR system focuses on detailed labelling to better explain risks and benefits, moving away from the simplicity of letter grades [6]. This change offers a more nuanced approach, paving the way for understanding Australia’s TGA system.
Australian Medication Safety Guidelines
Australia’s TGA builds on the FDA’s historical framework, offering a more detailed classification system tailored to local prescribing needs. The TGA uses an expanded alphabetical scale: A, B1, B2, B3, C, D, and X [4]. This approach differs significantly from the FDA’s former letter system, especially in how Category B is handled.
In the TGA system:
- Category B: Assigned when human data is unavailable, with subcategories based on animal study results:
- B1: No evidence of foetal harm in animals.
- B2: Inadequate animal data.
- B3: Evidence of potential risks in animals, though the significance for humans is uncertain [4].
- Category C: Identifies drugs with pharmacological effects that may cause reversible harm to the foetus but no malformations.
- Category D: Covers drugs linked to increased risks of foetal malformations or irreversible damage.
- Category X: Indicates drugs that pose a high risk of permanent harm and are contraindicated in pregnancy [4].
It’s important to note that the TGA explicitly warns that a B category doesn’t imply greater safety than a C category [4]. Category B reflects limited human data, while Category C is based on known or suspected pharmacological effects. Additionally, pharmaceutical companies in Australia may assign more restrictive classifications than the evidence suggests, often due to legal liability concerns [4].
The TGA’s database includes over 1,700 medications as of early 2025 [5], offering an extensive resource for dental professionals. For the most up-to-date recommendations specific to dental care, dentists should refer to the Therapeutic Guidelines: Oral and Dental Version 4, published in late 2025 [1] [3].
Safe and Unsafe Dental Medications During Pregnancy
Choosing the right dental medications during pregnancy is crucial for the health of both mother and baby. The Therapeutic Guidelines: Oral and Dental Version 4, updated in September 2025, provides essential guidance on this topic [1] [3]. Below, we explore the safety of local anaesthetics, antibiotics, and analgesics to help inform clinical decisions.
Local Anaesthetics and Pain Management
Local anaesthetics are considered safe for use during pregnancy and breastfeeding [2]. Notably, the 2025 guidelines now include articaine as an updated option for intermediate-acting local anaesthesia in nerve blocks [3]. This provides dentists with a reliable way to manage pain and treat infections without compromising safety.
For severe dental pain that doesn’t respond to oxycodone, tapentadol is suggested as an alternative, provided it complies with local regulatory requirements [3].
Antibiotics for Dental Infections
When it comes to dental infections, amoxicillin remains the go-to antibiotic for treating avulsed permanent teeth, backed by extensive clinical use [3]. For nonsevere spreading infections that can be addressed within 24 hours, penicillin monotherapy is recommended [3]. However, if treatment might be delayed, broader-spectrum options like penicillin combined with metronidazole or amoxicillin with clavulanate are advised to effectively target anaerobic bacteria [3].
For patients with penicillin allergies, the recommendations depend on the severity of their hypersensitivity:
- Cefalexin is suitable for those with mild to moderate penicillin allergies.
- Clindamycin is reserved for cases of severe hypersensitivity [3].
In situations where penicillin cannot be used, doxycycline is an alternative for managing avulsed teeth [3]. It’s important to note that untreated dental infections during pregnancy can lead to serious complications, such as pre-eclampsia, low birth weight, and premature delivery [2].
Analgesics and Sedatives: Risks and Alternatives
Non-drug approaches should always be the first choice for managing anxiety in dental patients [3]. When these methods are insufficient, minimal sedation options, such as benzodiazepines or short-term use of methoxyflurane, are considered acceptable [3]. The updated guidelines stress the importance of addressing the root cause of pain through dental procedures rather than relying heavily on medications. This approach not only reduces medication exposure but also ensures effective resolution of the problem.
These recommendations align with overarching best practices for dental care during pregnancy, prioritising both safety and effectiveness.
Best Timing for Dental Treatments During Pregnancy
Choosing the right time for dental treatments during pregnancy is crucial for ensuring both safety and comfort, especially when paired with updated medication protocols.
Second Trimester as the Preferred Period
The second trimester – spanning months 3 to 5 – stands out as the most suitable time for dental visits during pregnancy. By this point, the nausea and vomiting typical of the first trimester usually subside, and the gag reflex tends to improve [2]. According to the Australian Dental Association, "Trimester two of pregnancy may be the most comfortable to visit your dentist" [2].
During these middle months, most pregnant patients find it easier to sit or lie back in the dental chair without discomfort. By the third trimester, however, the growing baby’s size and weight can make reclining positions uncomfortable and may even lead to circulation issues [2]. This makes the second trimester an ideal time for routine procedures like professional cleanings and non-urgent treatments, as they are easier to manage for both patient and clinician.
While dental care is generally safe throughout pregnancy, extra care is needed during the first trimester. Dental Health Services Victoria points out that "Routine dental treatment is safe during pregnancy, although some procedures or medication should be avoided in the first 3 months" [7]. Scheduling non-urgent treatments for the second trimester ensures the patient’s comfort while allowing clinicians to deliver care effectively and with minimal risk.
Emergency Treatments: When and How
Although routine care is best suited for the second trimester, emergencies demand immediate attention, regardless of the pregnancy stage. Delaying treatment for severe dental issues can lead to serious complications, such as infections that increase the risk of premature birth and low birth weight [7]. The Australian Dental Association highlights this concern, stating that "Untreated tooth decay and gum disease can cause infections. These can be severe and a risk to you and your unborn baby" [2].
The updated 2025 guidelines underline the importance of prompt intervention for acute infections. For emergencies treated within 24 hours, penicillin monotherapy is recommended [3]. Acting quickly often allows for simpler treatment plans, while delays may necessitate broader-spectrum antibiotics [3]. For conditions like dental trauma, such as a knocked-out permanent tooth, amoxicillin is advised [3]. The takeaway is clear: addressing dental emergencies promptly during pregnancy safeguards both the mother and baby from the complications of untreated issues.
sbb-itb-2be92ed
Preventive and Non-Drug Approaches
Minimising the need for medications during pregnancy begins with consistent preventive care and maintaining good oral hygiene. The Australian Dental Association advises, "a general dental check-up is recommended for women who are considering becoming pregnant" [2]. By addressing existing issues like tooth decay or gum disease before conception, you can reduce the risk of emergencies that might require medication later. This proactive approach lays the groundwork for focusing on effective oral hygiene practices and non-drug pain management strategies.
Oral Health Maintenance During Pregnancy
Pregnancy brings hormonal changes that can make gums more sensitive to bacteria, often leading to pregnancy gingivitis. This condition, marked by red, swollen, and bleeding gums, can escalate to severe periodontitis if left unchecked. Such complications have been linked to premature birth and low birth weight [2][7]. To mitigate these risks, brushing twice daily with fluoride toothpaste and flossing every day are essential.
Morning sickness adds another layer of complexity. Vomiting introduces stomach acid to the mouth, which softens tooth enamel. Brushing immediately after vomiting can cause permanent enamel erosion. Instead, it’s best to wait 30 to 60 minutes before brushing [2][8]. During this waiting period, you can rinse your mouth with plain water, an alcohol-free fluoride mouthwash, or a mixture of one teaspoon of baking soda dissolved in a cup of water to neutralise the acid [2][7]. For immediate protection, applying a small amount of fluoride toothpaste to your teeth with your finger is a gentler alternative to brushing [2][8].
If a sensitive gag reflex makes brushing difficult, using a toothbrush with a small head and brushing later in the day when nausea subsides can help [2][8]. Additionally, adjusting your diet to include cheese, crackers, or plain yoghurt instead of sugary snacks can reduce the bacteria that cause decay. Drinking fluoridated tap water regularly also provides added protection for your enamel [2][7].
Non-Drug Pain Management Techniques
Managing dental anxiety without resorting to medications is another way to protect both maternal and foetal health. According to the latest Therapeutic Guidelines, "To manage anxiety in dentistry, nonpharmacological strategies have been added as the first-line approach" [3]. This shift encourages dental professionals to focus on behavioural methods before considering sedatives. Techniques like slow nasal breathing during procedures, distraction methods, and scheduling appointments at times when you feel most at ease can significantly reduce dental anxiety.
Chewing sugar-free gum between meals is another simple yet effective strategy. It stimulates saliva production, which naturally neutralises acids and helps clear away food particles [2][7]. Together, these approaches create a comprehensive, medication-free plan for maintaining oral health and managing discomfort during pregnancy.
Clinical Assessment and Collaborative Care
Treating pregnant patients requires a systematic approach that combines thorough information gathering and close coordination with the healthcare team. The Therapeutic Guidelines: Oral and Dental Version 4, released digitally in late 2025, now includes detailed recommendations for addressing oral health concerns in pregnancy. The guidelines highlight that "comorbidities are crucial considerations in planning dental treatment" (Therapeutic Guidelines) and stress that pregnancy is a unique physiological state requiring careful evaluation [3]. This initial assessment forms the basis for a comprehensive medical history review.
Medical History Review
Before starting any treatment, it’s essential to confirm the patient’s pregnancy status, determine the trimester, and evaluate any pre-existing conditions such as obesity, kidney or liver failure, cancer, or neurological disorders. This ensures that dental care is tailored to the patient’s specific needs. Document all current medications and check for antimicrobial hypersensitivities, especially to penicillin. The updated guidelines offer clarity by distinguishing between nonsevere and severe penicillin hypersensitivity. Additionally, assess risks for complications like periprocedural bleeding, infective endocarditis, surgical-site infections, or adrenal crisis. The digital guidelines include quick-reference tables to help classify risks efficiently during consultations.
Working with Obstetricians
After completing the patient assessment, collaboration with obstetricians becomes essential, particularly when uncertainties arise. If there are questions about the safety of specific medications or how systemic health conditions might influence dental procedures, consulting the patient’s obstetrician is key. The Therapeutic Guidelines: Oral and Dental Version 4 reinforces this in its section, "Guidance for medical practitioners managing oral and dental issues", which underscores the importance of addressing the unique requirements of pregnant patients [3]. This shared resource fosters effective communication between dental and medical professionals, ensuring coordinated care. Make use of digital tools for real-time drug guidance and procedural flowcharts when dealing with acute odontogenic infections, aiming to safeguard both the patient’s oral health and pregnancy outcomes.
Conclusion
The upcoming release of the Therapeutic Guidelines: Oral and Dental Version 4 in late 2025 introduces updated, evidence-based protocols designed to ensure the safety of both mothers and their unborn babies. These guidelines reaffirm that dental treatment during pregnancy is not only safe but also essential when necessary. Ignoring dental issues like decay or gum disease can lead to serious risks, including pre-eclampsia, low birth weight, and premature births [2].
Timing plays a key role in achieving the best outcomes. Routine dental care is most suitable during the second trimester (months 3 to 5), while emergencies should be addressed immediately, regardless of the stage of pregnancy.
Clear and effective communication is another cornerstone of these guidelines. Dentists are encouraged to collaborate with obstetricians when questions arise about medications or broader health concerns. The digital format of the new guidelines supports this teamwork by providing instant access to drug safety information and step-by-step procedural charts during patient care.
The inclusion of refined antibiotic stewardship, articaine for nerve blocks, and tapentadol as an option for severe pain management offers dental professionals greater flexibility to tailor treatments to individual needs [3].
Embracing these digital-first guidelines ensures decisions are made based on the latest evidence. As the Australian Dental Association highlights, "As scientific evidence‐based guidelines, their greatest value is being kept up to date" [1]. This approach empowers practitioners to deliver care that prioritises the health and safety of both mother and baby through informed, collaborative efforts.
FAQs
What dental medications are safe to use during pregnancy?
When it comes to dental medications during pregnancy, the focus is always on safety. Medications in the lower-risk Australian pregnancy categories (A, B1, or B2) are typically considered safe for use. For managing pain, paracetamol (Category A) is the go-to choice for mild to moderate discomfort. If a bacterial infection arises, penicillin-based antibiotics like amoxicillin or phenoxymethyl-penicillin (Category A/B1) are often recommended. When additional treatment for anaerobic bacteria is required, metronidazole or clindamycin (both Category B1) can be used after the first trimester.
Local anaesthetics such as lidocaine, prilocaine, and articaine are also deemed safe when administered in standard doses. These have been widely used in pregnant patients without evidence of increased risks to pregnancy.
On the other hand, certain medications should be avoided due to their higher-risk classifications (C, D, or X). These include tetracyclines, fluoroquinolones, high-dose aspirin, and ibuprofen after 30 weeks of pregnancy. It’s always crucial to consult your healthcare provider or refer to the Therapeutic Goods Administration (TGA) guidelines to ensure the safety of any medication during pregnancy.
Why is the second trimester the safest time for dental treatments during pregnancy?
The second trimester is generally considered the best time for dental treatments during pregnancy. By this point, early pregnancy symptoms such as nausea and vomiting usually ease up, and the baby’s major organs are fully formed. Plus, the uterus remains small enough to allow for more comfortable positioning in the dental chair. This period provides a great opportunity to handle any needed dental care while keeping both the mother’s and baby’s well-being in mind.
What are the differences between the TGA and FDA pregnancy drug safety classifications?
The Therapeutic Goods Administration (TGA) in Australia classifies medicines used during pregnancy into categories – A, B1, B2, B3, C, D, and X. This system is designed to help healthcare providers evaluate the potential risks these medications may pose to both the mother and the unborn baby.
By comparison, the US Food and Drug Administration (FDA) once used a similar letter-based system but has since adopted a narrative labelling approach. This updated method offers detailed guidance on the risks, benefits, and clinical considerations of using medications during pregnancy. While both systems share the same goal – ensuring safe prescribing practices – the TGA’s categorisation remains specific to Australia.
Related Blog Posts
- Is Tooth Extraction Safe During Pregnancy?
- Oral Infections and Preterm Birth: 1st vs. 3rd Trimester
- Pregnancy and Restorative Dental Work: Pros and Cons
- Is Local Anesthesia Safe During Pregnancy?
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





