







Periodontal Disease vs. Cardiovascular Risk: Analysis

Periodontal disease, a common gum condition, is linked to a higher risk of heart issues like heart attacks and cardiovascular disease (CVD). Studies show that people with gum disease may face a 20–25% increased risk of CVD, although the connection could partly stem from shared factors such as smoking, diabetes, and low socioeconomic status. While gum disease treatment improves markers like inflammation, there’s no solid proof yet that it prevents heart attacks or strokes.
Key points:
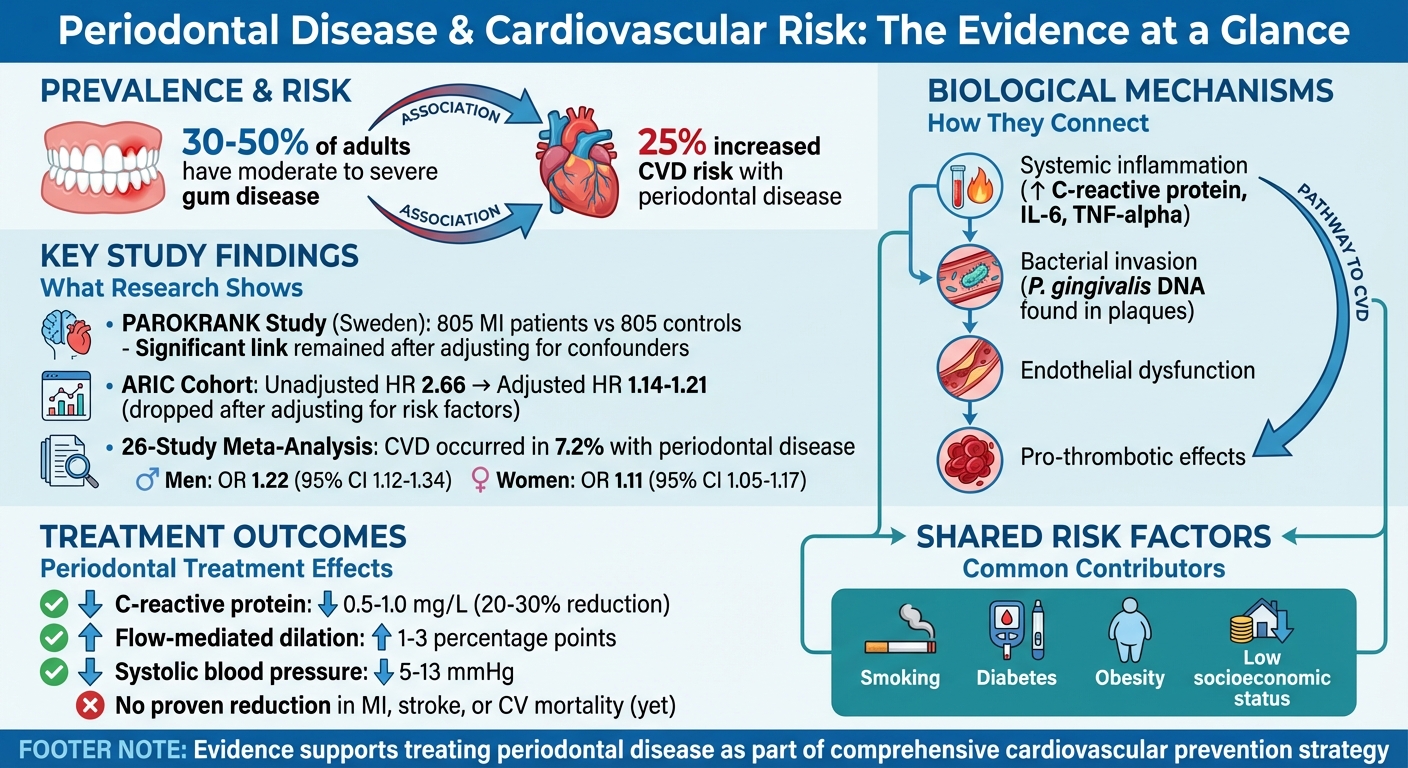
- Prevalence: 30–50% of adults have moderate to severe gum disease.
- Risk Increase: Gum disease raises CVD risk by around 25%.
- Biological Link: Inflammation and bacteria from gum infections may affect blood vessels and the heart.
- Treatment Impact: Improves health markers like blood pressure but lacks evidence for reducing CVD events.
- Shared Risks: Smoking, diabetes, and obesity affect both conditions.
For Australians, integrating oral health into overall health checks could help manage risks, especially for vulnerable groups like older adults, smokers, and Indigenous communities.
Periodontal Disease and Cardiovascular Risk: Key Statistics and Evidence
Perio & Cardio animation
Population Studies Linking Periodontal Disease and Heart Disease
Over the last two decades, researchers have conducted extensive studies to explore the connection between periodontal disease and cardiovascular health. These efforts include large-scale prospective cohort studies tracking thousands of participants over time and case–control studies comparing heart attack patients with healthy individuals.
One standout example is the PAROKRANK study from Sweden, which examined 805 first-time heart attack (MI) patients alongside 805 matched controls. Participants were paired based on age, sex, and location [1]. The study used radiographic bone loss as a reliable indicator of cumulative periodontal damage to identify moderate to severe periodontitis. Even after adjusting for confounding factors like smoking and abnormal blood glucose levels, the presence of moderate to severe gum disease remained closely linked to an increased risk of a first heart attack [1][4]. This finding suggests that periodontal disease could independently contribute to heart attack risk, beyond shared lifestyle factors.
On the other hand, a major cohort analysis published in JAMA followed 1,265 coronary heart disease (CHD) events. Initially, the unadjusted hazard ratio was 2.66, but it dropped to 1.14 (95% CI 0.96–1.36) or 1.21 (95% CI 0.98–1.50) after adjusting for confounders [2]. This significant reduction led researchers to conclude that much of the observed relationship was likely due to shared risk factors, rather than a direct causal link [2].
A 2023 systematic review and meta-analysis combined data from 26 observational studies, showing that cardiovascular disease occurred in 7.2% of individuals with periodontal disease. The odds ratios were 1.22 (95% CI 1.12–1.34) for men and 1.11 (95% CI 1.05–1.17) for women [3]. Notably, the results showed no major differences between sexes, and the association remained consistent across sensitivity analyses [3]. These findings align with the broader trend seen in individual studies. International consensus reports estimate that periodontitis increases the risk of cardiovascular disease, particularly heart attacks, by around 25% [4][5].
Key Study Comparisons
| Study / Review | Design & Population | Periodontal Measurement | Cardiovascular Outcome | Adjusted Risk Estimate |
|---|---|---|---|---|
| PAROKRANK (Sweden) [1] | Case–control; 805 first-MI patients, 805 matched controls | Radiographic bone loss; moderate–severe periodontitis | First myocardial infarction | Increased odds of first MI with moderate–severe periodontitis, adjusted for smoking, glucose levels, etc. |
| ARIC-based cohort (JAMA) [2] | Prospective cohort; 1,265 CHD events over follow-up | Clinical periodontitis categories (healthy, gingivitis, periodontitis) | Composite CHD events (fatal/non-fatal, revascularisation) | Unadjusted HR 2.66 (95% CI 2.34–3.03); adjusted HR 1.14 (95% CI 0.96–1.36) or 1.21 (95% CI 0.98–1.50) |
| 26-study meta-analysis [3] | Systematic review & meta-analysis of observational studies | Various clinical periodontitis definitions | Any CVD; CHD; stroke; heart failure; hypertension | Men: OR 1.22 (95% CI 1.12–1.34); Women: OR 1.11 (95% CI 1.05–1.17) for CVD in periodontitis vs non-periodontitis |
| Consensus reviews [4][5] | Multiple cohort and meta-analyses | Varied (clinical attachment loss, radiographic bone loss) | Coronary heart disease, myocardial infarction | ~20–25% increased relative risk after adjustments |
These studies collectively point to a modest but consistent link between periodontal disease and cardiovascular conditions. The strength of this connection often depends on how gum disease is measured and the degree of adjustment for confounding factors. For instance, studies using objective methods like radiographic bone loss tend to show stronger associations, while those relying on self-reported gum health or incomplete data often reveal weaker links after adjustments [3][5]. These findings pave the way for further research into the biological mechanisms driving this relationship.
How Gum Disease May Affect Heart Health
Emerging research highlights a connection between chronic gum infections and cardiovascular health, revealing several biological pathways that may link the two. A key player in this relationship is systemic inflammation. Chronic periodontitis triggers an increase in inflammatory markers like C‑reactive protein, interleukin‑6, and tumour necrosis factor‑alpha. These markers can harm the inner lining of blood vessels, encourage fatty plaque build-up, reduce nitric oxide (important for blood vessel function), and elevate oxidative stress. Together, these processes are known to set the stage for atherosclerosis.
Scientists are now delving deeper into how these mechanisms work at the cellular level. Another significant pathway involves the direct invasion of bacteria. Everyday actions such as chewing or brushing your teeth can allow periodontal bacteria, such as Porphyromonas gingivalis, to enter the bloodstream – a phenomenon called bacteraemia. Researchers have even found DNA from these bacteria in atherosclerotic plaques and heart valve tissues. This repeated bacterial entry from periodontal pockets has been linked to an increased risk of heart issues, supporting earlier findings from population-based studies [1].
Other potential mechanisms include immune cross-reactivity, where the body’s antibodies against bacterial proteins mistakenly attack similar proteins in blood vessels, and pro-thrombotic effects, where bacterial products promote clot formation and negatively affect lipid levels. While these mechanisms are considered plausible by periodontal and cardiology experts, definitive causation remains under investigation.
The connection between gum disease and heart health is also strengthened by shared risk factors like smoking and diabetes, which are known to contribute to both conditions.
| Mechanism Type | Key Features | Strengths of Evidence | Limitations/Uncertainties |
|---|---|---|---|
| Direct biological (bacterial & inflammatory) | Periodontal bacteria can enter the bloodstream and colonise blood vessels; chronic infection raises inflammatory markers, damages the endothelium, and promotes clotting. | Bacterial DNA has been identified in atherosclerotic plaque, and studies like PAROKRANK suggest a link with heart attacks. | Most evidence is observational, with limited randomised trials examining direct cardiovascular outcomes. |
| Indirect behavioural (shared risk) | Lifestyle factors such as smoking, diabetes, poor diet, and low socioeconomic status increase the risk of both gum and heart diseases. | Strong data supports these lifestyle factors as contributors to cardiovascular disease. | This explanation doesn’t fully account for the residual heart risk seen after adjusting for other factors. |
For Australian clinicians, these findings highlight the importance of factoring gum health into cardiovascular prevention strategies, particularly for patients with conditions like diabetes or a smoking history. Dental practices such as Complete Smiles Bella Vista can play a vital role in this integrated care model by providing thorough periodontal assessments, non-surgical treatments, and ongoing maintenance. Collaborating with general practitioners and cardiologists ensures a more comprehensive approach to patient care, reinforcing the need for a team effort in managing overall health.
Does Treating Gum Disease Reduce Heart Disease Risk?
The connection between treating gum disease and reducing the risk of heart attacks or strokes is still not fully understood. Research, including multiple randomised controlled trials, has shown that intensive periodontal therapy – such as scaling and root planing – can improve cardiovascular biomarkers in just a few months. For instance, studies have found reductions in high-sensitivity C-reactive protein levels by approximately 0.5–1.0 mg/L (a drop of around 20–30% from baseline), improvements in flow-mediated dilation by 1–3 percentage points, and decreases in systolic blood pressure ranging from 5–13 mmHg after treatment [4]. These changes, which indicate lower inflammation and better vascular function, are linked to a reduced risk of cardiovascular problems. However, whether these improvements translate into fewer heart attacks or strokes over time remains uncertain.
To date, no large-scale trial has definitively proven that periodontal therapy can prevent major cardiovascular events like heart attacks, strokes, or cardiovascular-related deaths [3][4]. Most studies in this area have been small and short-term, with follow-up periods ranging from weeks to about a year – far too brief to observe long-term heart health outcomes. Observational studies have also been inconclusive [3][4].
Experts in periodontology and cardiology worldwide agree there is a consistent link between gum disease and heart health, supported by plausible biological mechanisms. However, they stop short of asserting that periodontal treatment can prevent cardiovascular events [4][5]. Current guidelines recommend treating gum disease to improve oral health and quality of life, with any cardiovascular benefits considered a potential but unproven bonus [4][5].
In light of this evidence, Australian healthcare providers should include periodontal care as part of a broader strategy to reduce cardiovascular risks. Dentists are encouraged to screen patients with moderate to severe gum disease for cardiovascular risk factors – such as smoking, diabetes, or high blood pressure – and refer them for medical evaluations when necessary. General practitioners and cardiologists should ensure their patients with heart disease or significant risk factors receive regular periodontal check-ups and professional cleanings, often every three to six months. Dental practices, like Complete Smiles Bella Vista, can play a key role by incorporating periodontal assessments and structured maintenance programs to support overall cardiovascular health [3][4].
Patients should be informed that maintaining good periodontal care benefits overall health and may improve cardiovascular function. However, the most reliable ways to lower cardiovascular risk remain well-established measures: quitting smoking, staying physically active, eating a heart-friendly diet, managing blood pressure and cholesterol, and taking prescribed medications. These should be paired with regular dental visits and diligent oral hygiene at home [3][4]. Large, long-term studies will be necessary to move from understanding associations and mechanisms to making clear recommendations in Australian cardiovascular and dental guidelines [3][4].
sbb-itb-2be92ed
Guidance for Dentists and Doctors
To effectively manage patients at risk of both periodontal disease and cardiovascular conditions, dentists and doctors in Australia need to work together. Dentists should incorporate a quick medical risk screening into periodontal assessments. This could include checking blood pressure, smoking status, diabetes, BMI or waist circumference, and family history. If moderate to severe periodontitis is identified, dentists should document these findings and notify the patient’s GP or cardiologist. This notification should recommend a cardiovascular risk assessment in line with Australian guidelines, such as an absolute cardiovascular disease (CVD) risk assessment for adults aged 45 and older, or from 35 years for Aboriginal and Torres Strait Islander peoples [1][3][4][5]. This collaboration paves the way for medical professionals to consider oral health as part of a broader health evaluation.
On the medical side, practitioners should keep an eye out for gum-related symptoms like bleeding, loose teeth, or bad breath, and also monitor how regularly high-risk patients visit the dentist [1][3][4][5]. If poor oral health or infrequent dental care is evident, GPs and cardiologists should encourage a thorough dental check-up and periodontal treatment. Periodontal disease should be noted as a chronic inflammatory condition in the patient’s medical records. This is particularly relevant when addressing shared risk factors like smoking, diet, and diabetes, as these can heighten the risks for both periodontal and cardiovascular diseases.
For Aboriginal and Torres Strait Islander peoples, who face a greater burden of both periodontal and cardiovascular conditions, early and culturally appropriate referrals are critical. Screening and referrals should occur earlier, starting at around age 35, with a focus on preventive care [3][4][5]. Care should be delivered in a culturally safe manner, often in partnership with Aboriginal Community Controlled Health Services. Local health workers play a key role in encouraging attendance and explaining the connection between gum health and heart health in simple terms. Medical teams should also integrate dental care into chronic disease management plans, addressing barriers like transport, cost, and housing that may hinder access to care.
A two-way referral system can strengthen this collaborative approach. Dentists should refer high-risk periodontal patients to GPs for cardiovascular risk assessments, while GPs should direct patients with cardiovascular disease to dentists for periodontal evaluations. Standardised referral templates can streamline this process [3][4][5]. Shared care plans involving dentists, GPs, and cardiologists can focus on key areas such as smoking cessation, blood sugar control, and periodontal therapy. Research shows that periodontal treatment can improve markers like C-reactive protein and endothelial function, further highlighting the importance of this partnership. Coordinated recall systems with three- to six-monthly periodontal reviews, aligned with chronic disease care plans and medication reviews, can help patients stay on track with both dental and medical treatments.
Local dental practices can also play a vital role by incorporating cardiovascular screening into routine check-ups. Establishing formal ties with local GP and cardiology practices through referral protocols and participating in multidisciplinary case discussions can ensure care for high-risk patients is well-coordinated and consistent with national cardiovascular prevention strategies [1][3][4][5].
Pros and Cons
The connection between periodontal disease and cardiovascular risk has been explored extensively, revealing both strengths and limitations in the evidence. Numerous cohort studies, case–control analyses, and meta-analyses have found positive associations across different regions and genders [3][4][5]. For example, the PAROKRANK case–control study, which involved 805 first-myocardial-infarction patients and matched controls, showed that moderate to severe periodontitis was still significantly linked to myocardial infarction (MI) after adjusting for major confounding factors [1]. Expert consensus suggests periodontitis could increase overall cardiovascular disease (CVD) risk by approximately 25% [4][5]. The biological basis for this link is also compelling: periodontal treatment has been shown to lower systemic inflammatory markers, like C-reactive protein, and improve endothelial function, which supports the idea of a pathway between gum inflammation and heart disease [1][4].
However, the ability to establish a direct cause-and-effect relationship is limited by confounding factors. Much of the evidence is observational, making it difficult to separate the impact of periodontal disease from shared risk factors like smoking, diabetes, obesity, and socioeconomic status [3]. For instance, in the ARIC cohort study, the unadjusted hazard ratio for coronary heart disease in individuals with periodontitis was 2.66, but this dropped to 1.14–1.21 and lost statistical significance after accounting for cardiovascular risk factors [2]. Additionally, studies vary in how they define periodontal disease – whether through clinical criteria, radiographic bone loss, or self-reported data – introducing inconsistencies that can either dilute or exaggerate the observed associations [3][5].
Another major limitation is the absence of long-term randomised controlled trials (RCTs) that track cardiovascular outcomes. While the biological plausibility of a link between periodontal inflammation and heart disease is strong, definitive clinical evidence is lacking. Periodontal treatment has been shown to improve surrogate markers, such as inflammation and endothelial function, but no large-scale, long-term trials have demonstrated reductions in myocardial infarction, stroke, or cardiovascular mortality [3][4]. Current mechanistic data rely on these surrogate outcomes rather than actual cardiovascular events, making it difficult to prove that treating gum disease will directly prevent heart attacks or strokes. Expert groups agree there is a robust association with biological plausibility, but the lack of definitive proof leaves the question of causality unresolved [4][5].
The following table summarises the strengths and weaknesses of the current evidence:
| Aspect | Strengths | Weaknesses |
|---|---|---|
| Study consistency and volume | Multiple cohort, case–control, and meta-analytic studies show positive associations across regions and genders [3][4][5] | Effect sizes are modest (OR ~1.1–1.2) and may disappear after rigorous adjustment [2][3] |
| Control of confounding | Several large studies adjust for traditional risk factors like smoking, diabetes, and blood pressure [1][3] | Residual confounding from factors like smoking and socioeconomic status persists [2][3] |
| Biological plausibility | Chronic oral infection and inflammation plausibly contribute to systemic inflammation, endothelial dysfunction, and atherosclerosis; periodontal therapy improves biomarkers [1][4] | Mechanistic data rely on surrogate outcomes rather than actual cardiovascular events [4] |
| Strength of causal inference | Dose–response relationships and temporality are suggested in some longitudinal studies [1][3] | Evidence is mainly observational; few RCTs focus on CVD outcomes [3][4] |
| Long-term outcome data | Associations in large cohorts provide confidence that periodontal disease is a risk marker [3][4] | No large, long-term RCTs proving that periodontal treatment reduces MI, stroke, or cardiovascular mortality [3][4] |
For Australian clinicians and patients, the current evidence supports a practical, preventive approach. Maintaining good periodontal health as part of a broader strategy for managing cardiovascular risk makes sense – it’s low-risk and aligns with the principles of comprehensive care. This underscores the importance of collaboration between dental and medical professionals. Dental practices that prioritise thorough periodontal assessments can work closely with GPs and cardiologists to address shared risk factors, even as we await more definitive research [4][5]. These findings highlight the interconnected nature of oral and cardiovascular health, paving the way for more integrated care strategies.
Conclusion
The connection between periodontal disease and cardiovascular risk is supported by extensive research, though it falls short of proving direct causation. Moderate to severe periodontitis is linked to a slightly higher risk of cardiovascular disease – typically about 1.1 to 1.3 times greater – even after accounting for factors like smoking, diabetes, and blood pressure [1][3]. For instance, the PAROKRANK study found that periodontitis remained significantly associated with the first occurrence of myocardial infarction, even after adjusting for major confounders [1]. While large cohort studies confirm this modest link, they also reinforce that periodontal disease acts more as a risk marker than a direct cause [2][3][5].
Biological pathways further support this association. Chronic gum infections can lead to systemic inflammation, endothelial dysfunction, and bacteraemia, all of which contribute to the development of atherosclerosis [1][3][4]. Periodontal treatment has been shown to improve markers like C-reactive protein and endothelial function [1][4]. However, no large, long-term randomised controlled trials have definitively shown that treating gum disease reduces the risk of heart attacks, strokes, or cardiovascular mortality [3][4]. More research, particularly involving Australian populations, is needed to determine whether periodontal therapy can directly prevent cardiovascular events. This highlights the importance of integrating dental and medical evaluations.
For Australian clinicians and patients, the takeaway is straightforward: good periodontal health is a vital part of managing cardiovascular risk. Dentists should consider moderate to severe periodontitis as a potential indicator to discuss cardiovascular risk factors with their patients. Similarly, medical practitioners can include basic oral health questions in cardiovascular assessments and recommend regular dental visits, especially for individuals with diabetes, established cardiovascular disease, or those from Aboriginal and Torres Strait Islander communities, who experience higher rates of both conditions [3][4][5]. Practices like Complete Smiles Bella Vista exemplify this integrated approach, offering thorough periodontal care while collaborating with GPs and specialists to address shared risk factors.
Integrating dental and medical care provides a promising way to improve overall health outcomes. While oral health checks should complement – not replace – standard cardiovascular screening tools like blood pressure monitoring and lipid testing, they can offer additional insights into systemic inflammation and overall risk [3][4]. Collaboration between dentists, GPs, and cardiologists can be strengthened through shared correspondence, chronic disease management plans, and local referral networks, especially benefiting rural, remote, and socio-economically disadvantaged communities [3][5]. Together, these efforts create a comprehensive strategy for cardiovascular prevention.
The evidence supports managing periodontal disease as a key element of broader cardiovascular prevention. As research continues to shed light on causal pathways and the impact of interventions, Australian healthcare professionals have an opportunity to lead in providing coordinated care that acknowledges the deep connection between gum health and heart health, aligning with the collaborative model outlined above [4][5].
FAQs
What is the link between gum disease and heart health?
Gum disease, or periodontal disease, doesn’t just affect your mouth – it can also influence your heart health. When gums are inflamed, harmful bacteria can enter the bloodstream, potentially contributing to the build-up of arterial plaque. This increases the chances of heart disease and stroke.
Taking care of your oral health plays a key role in reducing these risks. Brushing, flossing, and scheduling regular dental check-ups, along with professional cleanings, are vital steps in preventing and managing gum disease effectively.
Can treating gum disease reduce the risk of heart attacks?
Managing gum disease, or periodontal disease, might play a role in lowering the risk of heart-related problems like heart attacks, though it’s not a foolproof solution. Studies highlight a link between oral health and heart health, indicating that treating gum disease could help minimise some risk factors associated with heart disease.
That said, keeping your heart in good shape requires more than just focusing on gum health. A well-rounded approach that includes eating a nutritious diet, staying active, and keeping up with regular medical check-ups is key to reducing cardiovascular risks.
What common factors link gum disease and heart disease?
Gum disease and heart disease have several shared risk factors, such as smoking, poor oral hygiene, diabetes, and an unhealthy diet. These factors can lead to inflammation and other health problems that impact both your mouth and your heart.
Taking care of your oral health by brushing and flossing regularly, eating a balanced diet, and making lifestyle changes like quitting smoking can lower the risks tied to both conditions. Don’t overlook the importance of regular dental check-ups – they’re key to keeping your gums healthy and catching potential issues early.
Related Blog Posts
- Best Practices for Periodontal Care in Cardiac Patients
- How Diabetes Impacts Periodontal Health Over Time
- Diabetes and Periodontitis: Oral Microbiome Changes
- Periodontal Disease in Lupus Patients: Key Facts
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





