







Periodontal Care for Patients with Disabilities

People with disabilities face a higher chance of developing periodontal disease due to challenges like reduced dexterity, medication side effects, and limited access to dental care. In Australia, barriers such as inaccessible clinics, long wait times, and high costs make preventive care difficult. This often leads to emergency-only treatment, worsening oral health outcomes.
Key takeaways:
- Disabilities can affect oral health through issues like dry mouth, poor plaque control, and difficulty using dental tools.
- Medications (e.g., anticonvulsants, antipsychotics) and high-sugar diets can increase risks of gum disease.
- Access issues include physical barriers, insufficient funding, and lack of trained professionals.
- Regular, tailored care – like scaling, fluoride treatments, and caregiver training – can improve outcomes.
Solutions include:
- Training caregivers in oral hygiene techniques.
- Using assistive devices like electric toothbrushes and floss holders.
- Scheduling frequent check-ups and collaborating with healthcare providers.
- Providing accessible facilities and flexible appointments.
With consistent and personalised care, oral health disparities for Australians with disabilities can be reduced, improving overall quality of life.
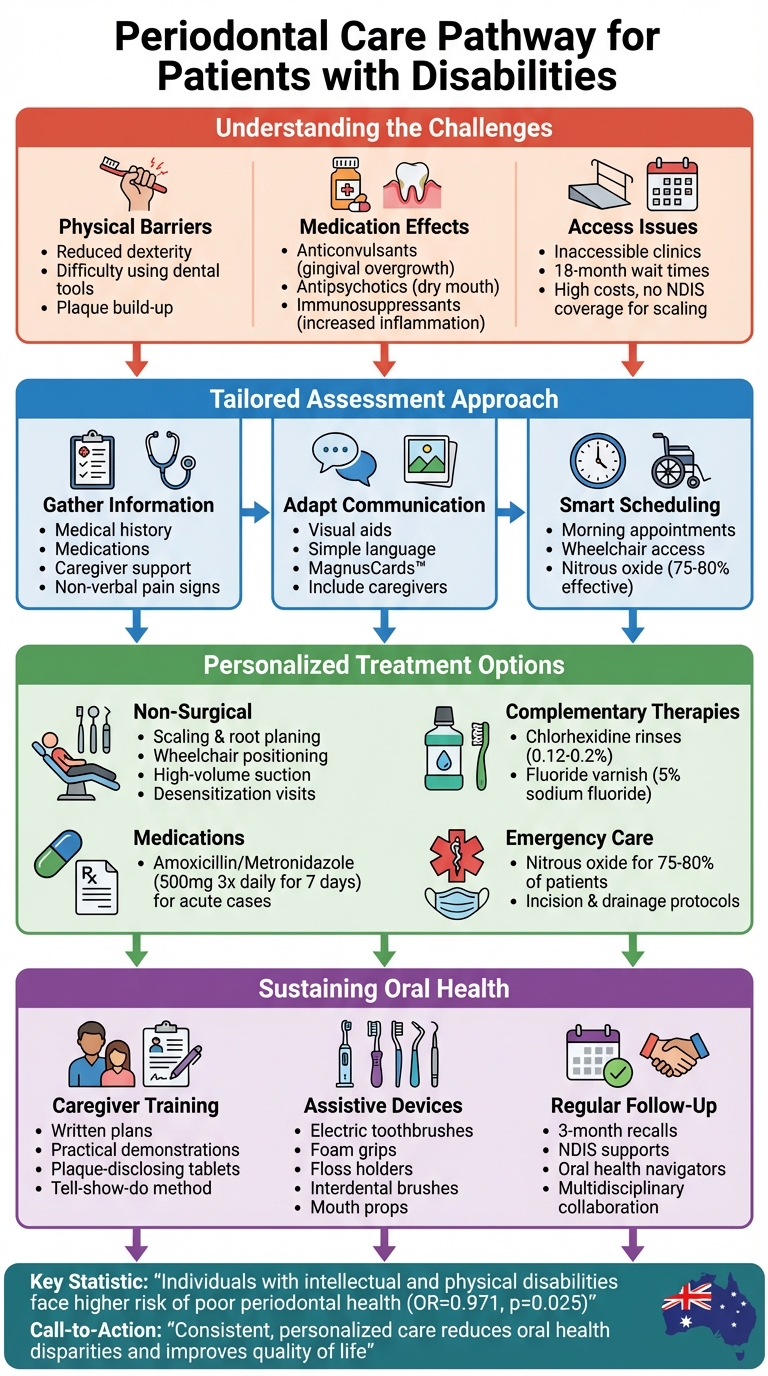
Comprehensive Periodontal Care Pathway for Patients with Disabilities
Risk Factors and Barriers to Periodontal Care
How Disabilities Affect Periodontal Health
Physical disabilities can make it difficult to handle toothbrushes and floss effectively, leading to plaque build-up, calculus formation, enamel erosion, and other issues like an increased gag reflex or malocclusion. These challenges often result in poor oral hygiene, which can escalate into more severe periodontal problems [5][3].
For individuals with intellectual and developmental disabilities, understanding and following oral hygiene instructions can be a significant hurdle. This often leads to higher levels of plaque biofilm. When intellectual disabilities are paired with physical impairments, maintaining oral health becomes even more challenging [5][2]. People with Down syndrome face additional hurdles, including reduced immunity, macroglossia (an enlarged tongue), crowded teeth, and dry mouth. These factors make plaque removal more difficult and increase the likelihood of developing periodontitis [5][3].
Sensory impairments add another layer of difficulty. They can make it harder to detect missed areas during brushing or to follow oral care instructions. This can result in poor biofilm control, which may worsen conditions like gingival hyperplasia. Combined with barriers to accessing care in the Australian healthcare system, these challenges can significantly impact oral health outcomes [5][2].
Access Barriers in the Australian Healthcare System
Accessing periodontal care in Australia comes with its own set of challenges. Many clinics are not equipped with essential features like wheelchair ramps or adjustable chairs, making them inaccessible for people with physical disabilities. For those living in regional areas, the lack of specialised care often means travelling long distances and enduring waiting periods that can stretch up to 18 months [1][2].
Cost is another major barrier. Critical periodontal treatments, such as scaling and root planing, are often not covered under NDIS funding. Public dental services are limited by strict eligibility requirements and long wait times, while private care is frequently unaffordable for many Australians. The lack of bulk-billing options and insufficient funding for adaptive equipment further complicate access to necessary care [1][2][7]. On top of these physical and financial barriers, managing treatment is made more difficult by the effects of medications and specific dietary needs.
Medication and Diet Effects on Oral Health
Certain medications can have a direct impact on oral health. For instance, anticonvulsants like phenytoin may lead to gingival overgrowth, creating pockets where plaque can accumulate. Antipsychotics and antidepressants often cause xerostomia (dry mouth), reducing saliva’s ability to protect teeth and gums. Additionally, immunosuppressants can worsen inflammation and raise the risk of periodontal disease [5][2].
Dietary habits can amplify these medication-related effects. For individuals with swallowing difficulties, modified-texture diets often include high-sugar foods, which encourage plaque adhesion and increase the risk of tooth decay. In institutional settings, frequent consumption of soft, sticky foods and caregiver-fed meals without proper oral cleaning can lead to persistent biofilm build-up, accelerating the progression of periodontal issues [5][2].
Assessment and Treatment Planning Methods
Gathering Medical and Social Information
Start by gathering a thorough understanding of the patient’s medical history, current medications, systemic conditions, physical abilities, living situation, and available caregiver support. For patients unable to communicate discomfort verbally, it’s critical to identify non-verbal signs of pain through discussions with caregivers before the appointment. This approach helps dental professionals create treatment plans that not only address clinical needs but also accommodate practical limitations.
Collaborating with other healthcare providers, such as general practitioners and social workers, can offer a more complete picture of how conditions like cerebral palsy or Down syndrome may impact periodontal health and treatment outcomes. Studies show that individuals with intellectual and physical disabilities are at a higher risk of poor periodontal health (OR=0.971, 95% CI=0.235–4.023, p=0.025) [2]. This highlights the importance of gathering comprehensive medical and social details to prevent complications and craft realistic, personalised care plans.
Communication and Consent Approaches
Once a detailed assessment is complete, adapting communication methods ensures that consent is both informed and clear. Use simple language, visual aids, and tools like MagnusCards™ to explain procedures in an accessible way [5].
Caregivers should be included in these discussions, but patient autonomy must remain a priority. For example, individuals with Down syndrome often understand more than they can express verbally [5][6]. Having caregivers present during explanations not only builds trust but also ensures that everyone involved fully understands the treatment plan. This collaborative approach helps overcome cognitive and behavioural challenges, creating a strong foundation for successful periodontal care.
These communication techniques also play a key role in managing behaviour and planning appointments.
Managing Behaviour and Scheduling Appointments
Clear communication leads seamlessly into effective scheduling strategies, which are essential for cooperative care. Short, morning appointments can help minimise anxiety and ensure patients are at their most comfortable and alert.
For patients with mobility challenges, such as those with cerebral palsy, ensure accessibility features like wheelchair ramps and adjustable seating are available. Nitrous oxide inhalation analgesia has been shown to work effectively for 75%–80% of patients, with sedation as an option for more complex cases [1].
Assigning an oral health navigator can further simplify the process. They can coordinate appointments, manage follow-ups, and connect patients to community resources, addressing common barriers to access. With regular, individualised visits, periodontal care becomes more manageable for both patients and their caregivers, fostering better long-term outcomes.
Treatment Techniques for Periodontal Disease
Adjusting Non-Surgical Periodontal Treatment
Scaling and root planing can still be highly effective when tailored to the needs of the patient. For individuals with cerebral palsy, ensuring wheelchair accessibility is crucial. Many dental professionals now treat patients while they remain in their wheelchairs, using portable headrests or wheelchair-tilt features to achieve safe working angles and reduce the risk of aspiration [3]. Stabilising the head and body helps manage involuntary movements, and shorter, well-timed appointments – scheduled when the patient is typically calm – can minimise fatigue.
For patients with challenges like drooling, dysphagia, or poor lip seal, high-volume suction becomes a necessity. When rubber dam isolation isn’t tolerated, cotton rolls, gauze, and frequent pauses can be used as alternatives [3][9]. In cases where noise sensitivity or pacemakers are a concern, hand instruments may be a better option, even though the process might take longer. To help anxious or autistic patients adapt, desensitisation visits can be introduced. These visits allow patients to familiarise themselves with the dental chair, instruments, and sounds before actual treatment begins, building trust and reducing anxiety over time [1][7].
Patients with Down syndrome often benefit from non-surgical periodontal therapy when the focus is placed on professional plaque control and managing inflammation, despite their immune system challenges [3][8]. Frequent maintenance visits and caregiver-supported home care are essential for achieving positive outcomes, rather than relying solely on modified clinical techniques. These adjustments lay the groundwork for incorporating additional therapies to further support periodontal health.
Complementary Therapies and Medications
In addition to mechanical treatments, adjunctive therapies can significantly improve results. Chlorhexidine gluconate rinses (0.12–0.2%) are particularly helpful when manual plaque control is difficult. For cooperative patients, rinsing and spitting is an option, while caregivers can assist non-verbal individuals by applying the solution with swabs [2][8]. Studies have shown that caregiver-administered chlorhexidine protocols, typically used for one to two weeks after scaling, improve periodontal health in individuals with intellectual disabilities.
High-concentration fluoride varnishes (5% sodium fluoride), applied professionally after scaling, help protect exposed root surfaces and reduce sensitivity, particularly in patients with Down syndrome [3][8]. For those experiencing xerostomia due to multiple medications – a common issue in this group – saliva substitutes, sugar-free lozenges, and high-fluoride toothpastes can support both periodontal health and cavity prevention [7].
For patients experiencing drug-induced gingival overgrowth from anticonvulsants, intensive plaque control with chlorhexidine rinses and thorough scaling is essential [2][4]. In some cases, coordination with the patient’s physician to explore alternative medications may be necessary. Systemic antibiotics like amoxicillin or metronidazole (500mg three times daily for seven days) are reserved for acute flare-ups, particularly in immunocompromised individuals, and are always paired with mechanical debridement [2][3].
Addressing Acute Periodontal Issues
When non-verbal patients present with acute periodontal infections, quick assessment is key. Caregiver insights and observation of facial expressions can help identify the problem. Immediate treatment often involves incision and drainage under local anaesthesia, with high-volume suction and short treatment bursts to minimise patient distress [1]. Tools like picture exchange systems or pain scales can assist in gauging discomfort when verbal communication isn’t an option.
Nitrous oxide inhalation is an effective option for about 75–80% of patients with disabilities who require pharmacological relaxation. This approach allows urgent treatment without the need for general anaesthesia [1]. Combined with trauma-informed care and familiar staff, nitrous oxide helps patients tolerate emergency procedures while building their confidence for future visits. Establishing clear protocols for urgent care – including designated contacts, prioritised appointment slots, and quiet treatment spaces – ensures that distressed patients receive prompt and compassionate attention when acute issues arise [1][7].
sbb-itb-2be92ed
Maintaining Periodontal Health Long-Term
Training Caregivers in Oral Hygiene
Daily plaque control is essential, and caregivers play a critical role in making it happen. To ensure success, effective training should include a written plan, practical demonstrations during dental visits, and regular monitoring using plaque-disclosing tablets. Clinicians can demonstrate proper brushing and interdental cleaning techniques, then observe caregivers as they practise these skills, providing tips on positioning and grip along the way [1][8].
Positioning is key. Whether caregivers are standing or sitting behind a patient – whether the patient is in a wheelchair or lying in bed – stabilising the head is crucial for accessing all tooth surfaces. Techniques such as the tell–show–do method can help build trust, starting with easier areas of the mouth and gradually incorporating oral hygiene into daily routines. Laminated step-by-step visual guides placed in bathrooms or staff areas can also serve as useful reminders for consistent care.
These hands-on strategies equip both patients and caregivers to use assistive devices effectively and adapt techniques as needed at home.
Assistive Devices and Modified Techniques
Caregiver training lays a strong foundation, but assistive devices can make daily oral care even more manageable. Tools like electric or oscillating–rotating toothbrushes are particularly helpful for individuals with limited manual dexterity, as they reduce the precision required for brushing. For those who find standard toothbrush handles challenging, modifications such as foam tubing, bicycle grips, or Velcro straps can improve control and encourage independence. Additional aids, including floss holders, interdental brushes, and soft picks, make cleaning between teeth easier, especially in areas with previous periodontal pockets [3][4][7][8].
For patients unable to rinse or spit effectively, a small smear of low-foaming toothpaste is recommended. Alternatives like chlorhexidine, applied using swabs or sprays, can also help maintain oral hygiene without the need for traditional rinsing. Mouth props can assist individuals with a strong bite reflex, but caregivers must be thoroughly trained in their safe use. Research shows that combining alcohol-free chlorhexidine with mechanical plaque control can significantly improve outcomes for high-risk patients.
Regular Follow-Up and Community Resources
Long-term periodontal health relies on personalised, risk-based recall schedules, often involving visits every three months or more frequently after treatment. These regular check-ups allow dental teams to reinforce home-care routines, perform professional plaque removal, and catch early signs of inflammation before they worsen.
In Australia, public schemes and NDIS supports provide essential resources for ongoing care [1][7]. Collaboration with GPs, speech pathologists, occupational therapists, and disability support services helps address challenges like diet, swallowing issues, and medication side effects. Some university clinics have even introduced oral health navigators to coordinate appointments, transport, and follow-ups, ensuring continuity of care. Private dental practices, such as Complete Smiles Bella Vista, also offer structured maintenance plans, caregiver training during visits, and referrals to specialists when needed.
Special Circumstances with Oral Hygiene for People with Intellectual/Developmental Disabilities
Conclusion
People with disabilities face higher rates of periodontal disease and often lack adequate dental care. Providing effective treatment means tailoring approaches to each individual’s needs. This could involve adjusting for physical challenges with modified positioning and specialised tools, or helping individuals with intellectual disabilities through visual aids and gradual desensitisation techniques. Personalised care is the cornerstone of achieving better outcomes [2][5][7].
Starting with early and tailored maintenance can help avoid more invasive procedures later. Regular periodontal care – such as frequent check-ups, customised plaque management, and caregiver education – can significantly lower the need for extractions or complex treatments under general anaesthesia. Studies show that structured preventive care improves plaque scores and ensures timely referrals when treatment is needed [2][5]. Beyond oral health, this proactive approach also supports better nutrition, reduces discomfort, and enhances overall quality of life, highlighting the importance of coordinated care.
Collaboration is key to effective periodontal treatment. Dental professionals, GPs, specialists, allied health workers, and disability support teams must work together to provide integrated care. Sharing information about medications that may affect saliva production or bleeding, consulting occupational therapists for patient positioning, and involving dietitians to improve nutrition are all crucial steps [2][5][7]. This teamwork ensures continuity of care and maximises outcomes. In Australia, public dental services, NDIS supports, and private practices like Complete Smiles Bella Vista offer accessible facilities, flexible appointment options, and consistent care to meet these needs.
Caregivers play a critical role in maintaining periodontal health. Training caregivers to assist with brushing, use adaptive devices, and identify early signs of oral health issues can make daily hygiene more effective [2][3]. Integrating these practices into existing care routines can lead to meaningful long-term improvements.
Accessible and patient-focused periodontal care is essential for achieving health equity for Australians with disabilities. By offering adaptive treatments, empowering caregivers, and fostering collaboration among healthcare providers, the disparity in periodontal outcomes can be addressed. When dental teams create inclusive environments and prioritise ongoing cooperation, they contribute to better systemic health and improved daily life for this underserved population [2][5][7].
FAQs
What are the best ways for caregivers to support oral hygiene for individuals with disabilities?
Caregivers play a vital role in maintaining oral hygiene by helping with daily brushing and flossing. Using tools like electric toothbrushes or floss holders can make the process easier, especially for those with limited mobility. It’s important to use gentle techniques and adjust the routine to match the individual’s abilities and comfort levels. This not only makes the experience more effective but also reduces stress for everyone involved.
Regular dental check-ups are equally important. Caregivers should consult dental professionals to learn specific techniques tailored to the person’s needs. A calm, supportive environment can also go a long way in addressing physical or behavioural challenges, making oral care a more comfortable experience.
What challenges do people with disabilities face when accessing dental care in Australia?
People with disabilities in Australia face several hurdles when it comes to accessing dental care. One major issue is physical accessibility – many clinics are not designed to accommodate wheelchairs or other mobility aids. On top of that, communication barriers can make visits difficult, especially for those with hearing, vision, or cognitive impairments.
Financial challenges also play a big role, as specialised dental treatments often come with high costs. Add to this the difficulty in finding transportation and the shortage of dental professionals equipped to cater to unique needs, and the situation becomes even more complex. Overcoming these barriers calls for targeted approaches to make oral health care accessible to everyone.
How can medications impact oral health in people with disabilities?
Medications can play a major role in oral health, particularly for individuals with disabilities. A frequent side effect is dry mouth, which lowers saliva production. This can create an environment where tooth decay and gum disease are more likely to develop. Additionally, some medications may change the makeup of saliva or lead to increased plaque build-up, compounding oral health concerns.
To counter these issues, regular dental check-ups and customised oral care routines are essential. It’s also a good idea to talk to your dentist or healthcare provider about the potential side effects of your medications. They can help you find ways to safeguard your oral health while managing your overall well-being.
Related Blog Posts
- How Medical Conditions Affect Gum Health in Seniors
- Checklist for Oral Care in Dementia Patients
- How to Teach Oral Care to Patients with Disabilities
- Training Caregivers in Elderly Oral Health
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





