







Differential Diagnosis: Drug-Induced Gingival Hyperplasia

Drug-induced gingival hyperplasia (DIGH) is a gum overgrowth caused by certain medications like anticonvulsants (e.g., phenytoin), immunosuppressants (e.g., cyclosporine), and calcium channel blockers (e.g., nifedipine). It typically starts in the small gum areas between teeth and may spread, disrupting speech, chewing, and oral hygiene. While DIGH is common, other gum enlargements can stem from inflammation, genetics, or systemic diseases like leukaemia. Misdiagnosis is frequent, with nearly half of cases mistaken for other conditions.
Key points:
- DIGH Appearance: Firm, pale pink, "mulberry-like" texture.
- Main Causes: Medications disrupting collagen breakdown.
- Differentiation: Inflammatory cases are softer and red; genetic forms are firm and leathery; systemic conditions often involve broader symptoms.
- Treatment: Switching medications, surgery, or addressing underlying issues like plaque or systemic health.
Accurate diagnosis is essential for effective treatment, as misdiagnosed cases can lead to severe complications.
Differential Diagnosis of Gingival Enlargement: Clinical Features and Characteristics
1. Drug-Induced Gingival Hyperplasia
Clinical Appearance
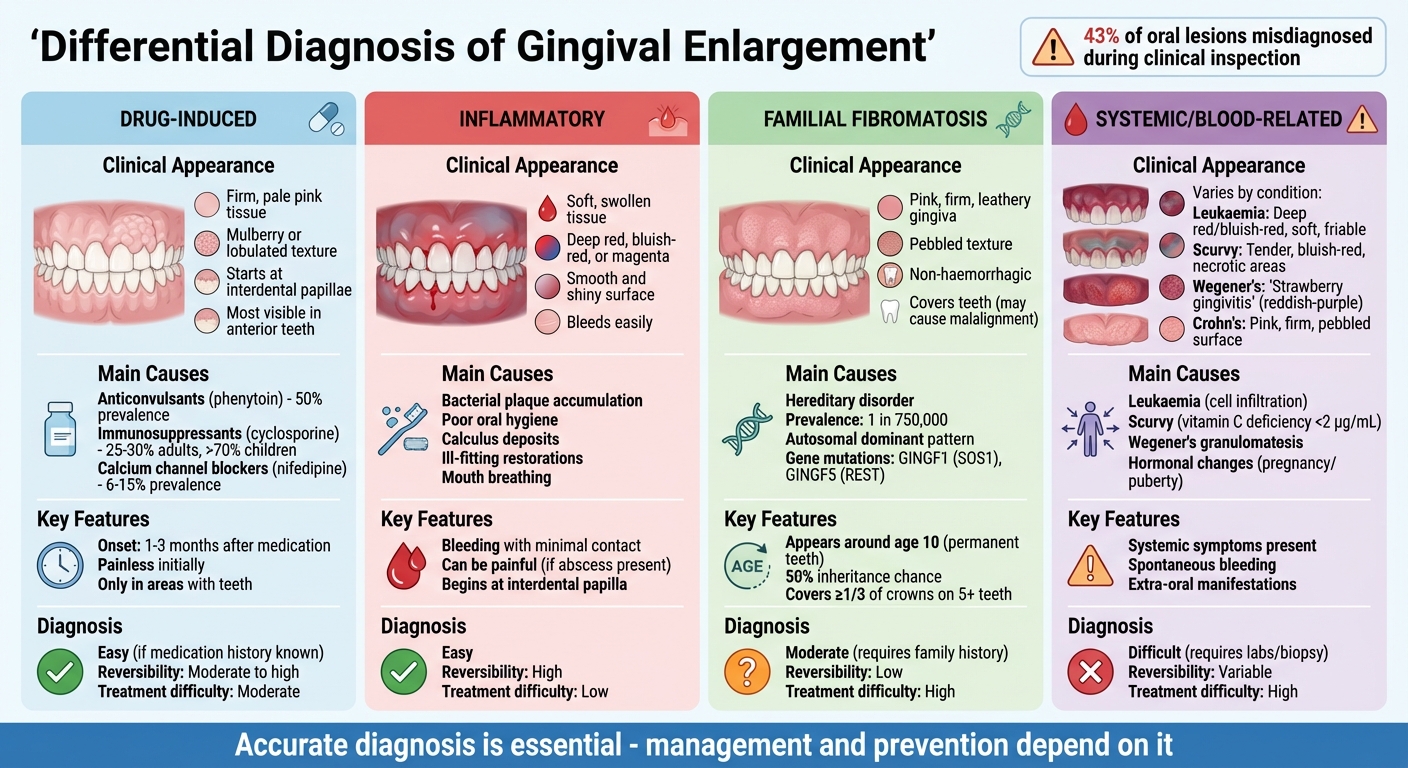
Drug-induced gingival hyperplasia presents as firm, pale pink gum tissue with a distinctive "mulberry" or lobulated texture [2][5][10]. The condition typically starts at the interdental papillae – the small triangular areas of gum between the teeth – and can gradually spread to cover parts of the tooth crowns [2][3]. It is most noticeable in the front teeth (anterior segment) and on the labial (lip-facing) surface [2][5]. Importantly, this overgrowth occurs only in areas where teeth are present. Edentulous (toothless) regions remain unaffected, and the condition tends to subside if the associated teeth are extracted [5][10]. These distinct characteristics often lead clinicians to review the patient’s medication history.
Aetiology
Three main classes of medications are linked to drug-induced gingival hyperplasia: anticonvulsants, immunosuppressants, and calcium channel blockers [4][5]. These drugs share a common mechanism – they block calcium influx, which disrupts collagenase activity [4][5].
| Drug Class | Common Examples | Estimated Prevalence |
|---|---|---|
| Anticonvulsants | Phenytoin, Sodium Valproate, Phenobarbital | ~50% [2][5][11] |
| Immunosuppressants | Cyclosporine A, Tacrolimus, Sirolimus | 25–30% (Adults); >70% (Children) [11] |
| Calcium Channel Blockers | Nifedipine, Amlodipine, Verapamil, Diltiazem | 6–15% (Nifedipine) [11] |
These medications stimulate certain fibroblast subsets, leading to the overproduction of extracellular matrix proteins and glycosaminoglycans [4][1]. Poor oral hygiene and gingival inflammation can worsen the condition [1][4]. Other contributing factors include younger age, male gender (for some drugs), and inadequate plaque control [2][9].
Associated Symptoms
Initially, the condition is painless, but severe cases can disrupt speech, chewing, and bite alignment. The enlarged tissue also makes oral hygiene challenging, often creating a cycle of poor plaque control, secondary inflammation, bleeding, and increased risk of periodontal disease [2][3][5][8]. Symptoms typically appear within 1 to 3 months of starting the medication [3][5]. These effects underscore the importance of a focused diagnostic approach.
Diagnostic Approach
"The diagnosis of drug-induced gingival overgrowth is mainly based on the clinical appearance of the gingivae and on the medical history." – European Association of Oral Medicine [2]
Diagnosis involves a detailed review of the patient’s medical history to identify the causative medication, paired with a clinical examination of the gums. This helps differentiate the condition from other periodontal diseases. Radiographs and periodontal assessments are used to rule out bone loss or other underlying issues [5]. In cases where the presentation is unusual or persistent, a biopsy may be performed to confirm the diagnosis and exclude the possibility of neoplastic changes [5]. If there is extensive bleeding, a Complete Blood Count (CBC) may be necessary to check for systemic conditions like leukaemia [5][10][11].
2. Inflammatory Gingival Enlargement
Clinical Appearance
Inflammatory gingival enlargement differs noticeably from drug-induced gingival hyperplasia. While drug-induced cases feature firm tissue, inflammatory enlargement is soft and prone to swelling due to local irritants. The affected tissue typically takes on a deep red, bluish-red, or magenta hue, a sharp contrast to the pale pink appearance of drug-related hyperplasia [13][4]. Its surface is smooth and shiny, bleeding easily during activities like brushing, eating, or even light contact [13][5].
The condition often begins with slight swelling of the interdental papilla or marginal gingiva [13]. For individuals who breathe through their mouth, the enlargement is usually confined to the anterior regions of the upper and lower jaws. In these cases, the gums appear red, swollen, and have a diffuse shiny surface, making it easier to differentiate from drug-induced cases [13].
Aetiology
The main culprit behind inflammatory gingival enlargement is bacterial plaque accumulation, often aggravated by poor oral hygiene [12][13]. Other contributing factors include calculus deposits, fractured teeth, improperly fitted dental restorations, ill-fitting prosthetics, and orthodontic brackets – all of which create favourable conditions for plaque retention [13]. Mouth breathing can also play a role by causing surface dehydration, though the exact process remains unclear [1][12]. The inflammation is driven by tissue oedema and infiltration of inflammatory cells, both triggered by prolonged exposure to plaque [12][13].
Associated Symptoms
One common symptom is bleeding with minimal contact [7]. In advanced cases, the tissue may become highly vascularised, leading to heavy bleeding [7]. Mouth breathers often show additional signs, such as a short upper lip and forward-angled incisors [13]. Unlike the painless onset of drug-induced gingival changes, acute inflammatory enlargement can be painful, especially if it indicates the presence of an abscess [13].
Diagnostic Approach
Diagnosis is primarily based on clinical examination, with a focus on identifying local irritants and observing how the tissue responds to plaque control efforts [13]. If scaling and root planing fail to reduce the enlargement, it could suggest a significant fibrotic component or an underlying systemic condition [12]. In cases of excessive bleeding, a Complete Blood Count may be required to rule out systemic issues [5]. These diagnostic steps are critical for distinguishing inflammatory gingival enlargement from other periodontal conditions discussed in later sections.
3. Familial Gingival Fibromatosis
Clinical Appearance
Familial gingival fibromatosis is an inherited condition that stands apart from drug-induced or inflammatory gingival enlargements. It typically presents with pink, firm, and leathery gingiva, which contrasts sharply with the soft, inflamed tissue seen in other types of overgrowth. The gingiva often has a pebbled texture, a feature that differentiates it from the mulberry-like appearance seen in drug-induced cases [4]. Unlike the bleeding and inflamed tissue of other forms, the gingiva in this condition is firm, pale, and non-haemorrhagic [14].
This overgrowth extends from the margin and interdental papillae into the attached gingiva, sometimes covering teeth and leading to issues like malalignment, diastemas (gaps between teeth), or delayed tooth eruption [14] [5]. It typically becomes noticeable when the permanent incisors erupt, usually around age 10, and is rarely seen in primary teeth [14]. These unique features often point to its genetic origin, prompting further investigation.
Aetiology
Familial gingival fibromatosis is a rare hereditary disorder, affecting about 1 in 750,000 people. It is primarily passed down through an autosomal dominant pattern [14]. Genetic mutations linked to this condition include changes in GINGF1 (a mutation in the SOS1 gene on chromosome 2p21) and GINGF5 (a mutation in the REST gene on chromosome 4q12) [14]. Unlike other forms of gingival overgrowth caused by medications, this condition is purely genetic – meaning an affected parent has a 50% chance of passing it on to their child [14].
"Hereditary gingival fibromatosis specifically occurs in the absence of other identifiable medical syndromes or medications known to cause gum overgrowth." – Dr. Delwyn Dyall-Smith [14]
Diagnostic Approach
Diagnosing familial gingival fibromatosis requires a thorough clinical examination and a detailed family history. A key diagnostic marker is gingival overgrowth covering at least one-third of the dental crowns of five or more teeth, combined with a positive familial history [14]. To rule out drug-induced enlargement, it’s crucial to confirm the patient is not taking systemic medications like phenytoin, cyclosporine, or calcium channel blockers [14] [5].
Histopathological analysis provides further clarity, showing dense fibrous tissue with thick collagen bundles and minimal blood vessels – a stark contrast to the inflammatory infiltrates seen in drug-induced cases [14] [6]. Due to its hereditary nature, genetic counselling is often recommended for individuals diagnosed with this condition [14].
4. Systemic and Blood-Related Conditions
Clinical Appearance
Systemic diseases bring their own distinct features to gingival enlargement, setting them apart from drug-induced and familial cases. For instance, drug-induced overgrowth typically presents as firm, pale pink tissue with a lobulated, mulberry-like surface [4]. In contrast, systemic conditions have more varied and striking appearances. Gingival tissue in leukaemia often looks deep red or bluish-red, soft, and friable, with mucosal pallor and a tendency for spontaneous bleeding [4][13]. Scurvy, caused by a lack of vitamin C, leads to tender, bluish-red gums that bleed easily and may even show areas of necrosis [5][10]. Wegener’s granulomatosis produces the characteristic "strawberry gingivitis", marked by reddish-purple swelling and petechial haemorrhages [10][13]. Crohn’s disease, on the other hand, is linked to pink, firm, leathery gingiva with a finely pebbled surface [10]. Pregnancy-related gingival changes are visually distinct, appearing bright red or magenta, smooth, shiny, and soft [10][11].
Aetiology
The causes behind these conditions are as varied as their presentations. In leukaemia, gingival enlargement arises from the infiltration of leukaemic cells, particularly in acute myeloid leukaemia [10]. Granulomatous inflammation is a hallmark of conditions like Wegener’s granulomatosis, sarcoidosis, and tuberculosis, contributing to gingival changes [4][10]. Scurvy occurs when serum ascorbic acid levels drop below 2 μg/mL, disrupting collagen synthesis and antioxidant defences [10]. Hormonal changes during pregnancy or puberty don’t directly cause enlargement but amplify the gingiva’s inflammatory response to plaque [10][11]. Unlike drug-induced cases, where the timeline of medication use is often clear, systemic conditions demand a deeper exploration of overall health.
Associated Symptoms
Systemic conditions frequently come with extra-oral symptoms, offering clues that help differentiate them from localised, drug-induced overgrowths. For example, leukaemia may present with fever, fatigue, night sweats, lethargy, and signs of bone marrow failure like ecchymoses [10][13]. Scurvy is marked by spontaneous bleeding and pronounced tenderness across the mouth [5][15]. Wegener’s granulomatosis often includes nasal bleeding and complications affecting multiple organs [13]. Plasma cell gingivitis, a rare condition, is associated with a burning sensation when consuming hot or spicy foods [10]. These broader symptoms are key in distinguishing systemic conditions from the typically painless, localised nature of drug-induced overgrowth.
Diagnostic Approach
"Accurate diagnosis is essential, as the management of these lesions and prevention of their recurrence is completely dependent on it." – Amit Arvind Agrawal [13]
Diagnosing systemic causes involves a more thorough approach compared to drug-induced cases. A Complete Blood Count (CBC) is often the first step to rule out conditions like leukaemia or anaemia [5][13]. Biopsies can provide crucial insights, such as identifying non-caseating granulomas or foreign body giant cells [5][10]. For sarcoidosis, chest X-rays are used to check for hilar lymphadenopathy, and serum angiotensin-converting enzyme (ACE) levels are assessed [10][13]. Scurvy is confirmed by measuring serum ascorbic acid levels, with a deficiency defined as less than 2 μg/mL [13]. Diagnosing Wegener’s granulomatosis requires meeting at least two criteria, such as detecting abnormal urinary sediment or granulomatous inflammation in a biopsy [13].
sbb-itb-2be92ed
Drug-Induced Gingival Enlargement | Complete Exam-Oriented Breakdown by Dr Chandni Sheik
Advantages and Disadvantages
Understanding the specific benefits and challenges of each type of gingival enlargement is key to accurate diagnosis and effective treatment. Each condition comes with its own set of complexities that can directly influence treatment success.
Drug-induced gingival hyperplasia is often easier to diagnose when a clear medication history is available. Medications like phenytoin, cyclosporine, and nifedipine are well-known contributors. Treatment outcomes vary widely – cyclosporine-induced overgrowth may subside once the drug is discontinued, but phenytoin-related cases often persist even after stopping the medication. A significant obstacle is that patients requiring these drugs, such as those managing epilepsy or recovering from organ transplants, may have no alternative therapies. Surgery is frequently needed, but recurrence is common within 3–6 months if the medication continues [5].
Inflammatory enlargement is generally straightforward to diagnose and responds well to professional cleaning and improved oral hygiene. However, familial gingival fibromatosis – easily identified through family history – usually necessitates surgical intervention and has a high likelihood of recurrence. Systemic conditions, on the other hand, are among the hardest to diagnose. Research shows that 43% of oral lesions are misdiagnosed during clinical inspection alone [3].
"A perfect diagnosis is critically important, since the management of these lesions and prevention of their recurrence is completely dependent on it" – Professor Amit Arvind Agrawal [13]
The following table highlights the key differences between these conditions:
| Condition Type | Ease of Diagnosis | Reversibility | Treatment Difficulty | Primary Challenge |
|---|---|---|---|---|
| Drug-Induced | Easy (if medication history known) | Moderate to high | Moderate | Requires medical coordination; high recurrence |
| Inflammatory | Easy | High | Low | Dependent on patient compliance with oral hygiene |
| Familial Fibromatosis | Moderate (family history required) | Low | High | Requires surgery; prone to recurrence |
| Systemic/Blood-Related | Difficult (requires labs/biopsy) | Variable | High | Mimics inflammatory changes; can be life-threatening if undiagnosed |
As shown, accurate diagnosis is vital. A combination of patient history, clinical examination, and collaboration with other healthcare professionals is crucial for effective management.
For drug-induced cases, interprofessional coordination is especially important. Dentists should consult with the patient’s physician before making any changes to medications. Allowing a 6–12 month period for resolution before considering surgery can significantly improve long-term outcomes. Additionally, maintaining strict plaque control is essential across all cases. Inflammation not only worsens gingival enlargement but also creates conditions that trap bacteria, perpetuating the cycle of tissue overgrowth.
Conclusion
Properly identifying the type of gingival enlargement is essential for effective treatment. Drug-induced gingival hyperplasia typically appears as firm, pink, mulberry-like tissue, starting around the interdental papilla. In contrast, inflammatory enlargement looks soft, deep red, and tends to bleed easily. Familial fibromatosis presents as non-tender, leathery overgrowth, while systemic conditions like leukaemia may cause diffuse swelling accompanied by other systemic symptoms.
Getting the diagnosis right is crucial. Studies indicate that 43% of oral lesions are misdiagnosed during clinical inspections, with cancerous lesions being incorrectly identified 5.6% of the time [3]. If you experience unusual gum swelling – particularly if you’re on medications such as phenytoin, cyclosporine, or calcium channel blockers, which are known to trigger gingival overgrowth – seek advice from a dental professional immediately. A thorough and timely evaluation can make all the difference.
In Australia, diagnostic services are readily available to provide detailed assessments and create tailored treatment plans. Alongside professional care, maintaining excellent oral hygiene plays a key role in managing all types of gingival enlargement. It can even help minimise the impact of drug-induced overgrowth, improving overall treatment outcomes.
FAQs
How can I tell if my gum overgrowth is medication-related or just gingivitis?
Medication-induced gum overgrowth tends to develop slowly and is associated with certain medications such as phenytoin, ciclosporin, or calcium-channel blockers. It usually manifests as firm, fibrous tissue with little to no inflammation. In contrast, gingivitis is characterised by red, swollen, and bleeding gums, often resulting from plaque buildup and poor oral hygiene. If you notice gum overgrowth after starting a new medication, it’s important to consult your dentist. They can assess your medical and medication history to provide a proper diagnosis.
Should I stop or change my medication if my gums start enlarging?
Always talk to your healthcare provider if you notice your gums starting to enlarge. They can determine if your medication needs to be adjusted or stopped and will guide you through this process safely. Making sudden changes to your medication without professional guidance can pose serious health risks.
What tests might a dentist request to rule out serious causes like leukaemia?
A dentist might suggest blood tests like a complete blood count (CBC) to check for serious conditions such as leukaemia. These tests give important insights into your blood cells and general health, helping to detect any underlying problems.
Related Blog Posts
- Types of Antibiotics for Gum Disease
- Differential Diagnosis for Periodontal Infections
- Research: Systemic Diseases Mimicking Periodontitis
- Differentiating Gum Cancer From Periodontal Disease
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





