







Dental Pulp Stem Cells in Regenerative Dentistry

Dental pulp stem cells (DPSCs) are transforming dentistry by enabling teeth repair and regeneration. Found in the soft tissue of teeth, these cells can differentiate into various types like odontoblasts, osteoblasts, and even neural cells. Unlike traditional methods that remove or replace damaged tissue, DPSCs aim to restore the tooth’s natural structure and function.
Here’s what you need to know:
- What are DPSCs? They are mesenchymal stem cells located in the dental pulp, capable of rapid self-renewal and differentiation. Their neurogenic origin makes them suitable for regenerating nerves and blood vessels.
- Why are they promising? DPSCs can be harvested from discarded teeth (e.g., wisdom teeth), are non-immunogenic, and retain functionality even after long-term cryopreservation.
- Clinical progress: Studies have shown successful regeneration of pulp tissue, nerves, and blood vessels in both children and adults. However, challenges remain, including regulatory hurdles, technical limitations, and patient variability.
- Applications: DPSCs are being explored for pulp-dentine regeneration, bone repair, and periodontal tissue restoration. Techniques include cell transplantation, cell homing, and the use of bioengineered scaffolds.
- Barriers to adoption: Strict regulatory standards, logistical challenges in cell collection, and the need for consistent protocols are slowing widespread clinical use.
While DPSCs are still in the research phase, their potential to improve outcomes in dental care is undeniable. From restoring vitality to teeth after root canal treatments to repairing craniofacial structures, these stem cells could change how we approach oral health care.
Biology and Sources of Dental Pulp Stem Cells
Biological Properties of DPSCs
Dental pulp stem cells (DPSCs) stand out because they originate from the cranial neural crest. This unique origin gives them enhanced neurogenic abilities, allowing them to transform into neurons and glial cells. These properties could play a role in repairing neural damage within the dental pulp [1][5]. DPSCs are incredibly versatile, capable of differentiating into various cell types such as odontoblasts, osteoblasts, chondrocytes, adipocytes, and endothelial cells. They also proliferate at a much faster rate compared to bone marrow stem cells [1][10][12][5].
"Dental pulp stem cells isolated from pulp tissue exhibit mesenchymal stem cell-like characteristics and are considered ideal candidates for regenerating damaged dental pulp tissue owing to their multipotency, high proliferation rate, and viability after cryopreservation."
– Kyu Hwan Kwack and Hyeon-Woo Lee, Department of Pharmacology, Kyung Hee University [1]
DPSCs also offer significant immunomodulatory benefits. They can suppress T-cell activity, encourage anti-inflammatory macrophages, and express low levels of Class II HLA-DR molecules, making them a promising option for transplantation without the need for strict donor–recipient matching [1][2]. Another important feature is their ability to maintain stemness and differentiation potential even after being cryopreserved for long periods, making them ideal candidates for cell banking [1][11].
With these impressive biological features in mind, let’s explore how DPSCs are sourced for regenerative purposes.
Sources of DPSCs
DPSCs are primarily harvested from teeth removed during routine dental procedures, such as impacted wisdom teeth, first premolars extracted for orthodontic reasons, and supernumerary teeth [1][5][10]. Instead of discarding these teeth, the pulp tissue inside can be utilised as a valuable source of stem cells.
There are two main methods to extract DPSCs:
- Enzymatic digestion: This method uses collagenase and dispase enzymes to isolate cells more quickly and yield higher initial cell counts.
- Explant culture: In this slower process, pulp tissue is cultured, allowing cells to migrate out naturally. Although time-consuming, it may better preserve cell-to-cell interactions [13][5][11].
For obtaining highly pure DPSC populations, techniques like cell sorting based on markers such as STRO-1, CD90, and CD146 are employed [13][3]. Once extracted, DPSCs or pulp tissue can be cryopreserved at ultra-low temperatures (around -196°C in liquid nitrogen) with the help of cryoprotective agents like Dimethyl Sulfoxide (DMSO) [1][10]. Remarkably, DPSCs remain viable even after extended periods of storage. For instance, teeth stored in phosphate-buffered saline at 4°C for up to 120 hours still yield viable cells, and cryopreserved DPSCs have shown an 85% survival rate after two years [10].
Other Dental Stem Cell Types
While DPSCs are a cornerstone of regenerative dentistry, other dental stem cell types also play vital roles. For example, Stem Cells from Human Exfoliated Deciduous Teeth (SHED), derived from baby teeth, show faster proliferation and stronger bone-forming abilities compared to adult DPSCs [3][12]. Clinical trials have even demonstrated that SHED can regenerate vascularised dental pulp and support the continued development of tooth roots [6].
Stem Cells from the Apical Papilla (SCAP) are another noteworthy group. With higher population doubling rates and more stemness markers like STRO-1, SCAP are particularly suited for regenerating tooth roots [12]. Meanwhile, Periodontal Ligament Stem Cells (PDLSCs) specialise in repairing cementum and the connective tissue that secures teeth to the jawbone [1][12].
Despite the contributions of these various stem cell types, DPSCs remain the preferred choice for regenerating the pulp-dentine complex due to their unmatched neurogenic and angiogenic capabilities [1].
Analysis of Human dental pulp Stem Cells | Protocol Preview
Applications of Dental Pulp Stem Cells in Regenerative Dentistry
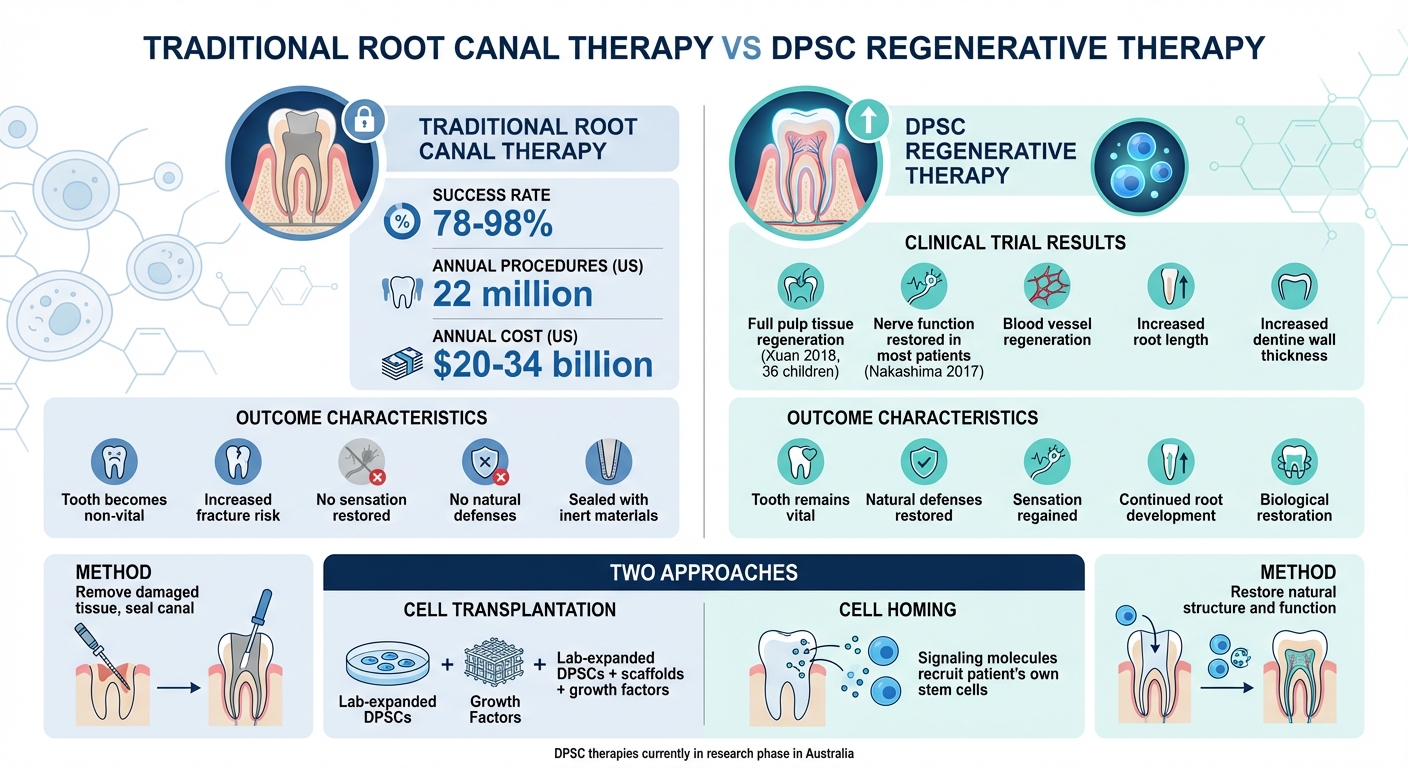
Traditional Root Canal vs DPSC Regenerative Therapy Comparison
Dental pulp stem cells (DPSCs) are making waves in regenerative dentistry, offering solutions that range from restoring damaged pulp tissue to repairing bone and soft tissues. Let’s explore how these tiny powerhouses are reshaping dental care.
Pulp-Dentine Complex Regeneration
Root canal therapy, with a success rate of 78–98%, is a common procedure for saving teeth. However, it leaves teeth non-vital and more prone to fractures. In the United States alone, around 22 million root canal procedures are performed annually, costing between $20 billion and $34 billion [8]. Instead of merely sealing the canal with inert materials, researchers are working on ways to restore the tooth’s vitality.
DPSCs offer a biological solution through two main approaches: cell transplantation and cell homing. In cell transplantation, DPSCs are isolated, expanded in a lab, and then implanted into the root canal using scaffolds (like collagen or hydrogels) combined with growth factors. Cell homing, on the other hand, leverages signalling molecules to recruit the patient’s own stem cells to repair the tissue – no external cells required.
A 2018 randomised clinical trial led by Kun Xuan studied 36 children aged 7–12 with necrotic permanent incisors caused by trauma. The experimental group received autologous SHED (stem cells from human exfoliated deciduous teeth) aggregates. Over 12 months, this treatment successfully regenerated full pulp tissue, including blood vessels and nerves, while also increasing root length and dentine wall thickness. This outperformed the traditional apexification method [8][14].
But DPSCs aren’t just about pulp regeneration – they’re also key players in repairing bone and craniofacial structures.
Bone and Craniofacial Regeneration
DPSCs are uniquely suited for bone regeneration because they originate from the cranial neural crest, the same embryonic tissue responsible for forming facial bones and the skull [7][15]. This shared origin gives DPSCs a natural edge in forming bone tissue.
"The osteoblasts in the craniofacial region are also derived from neural crest cells… Therefore, DPSCs have great osteogenic potential."
– Ye Liu et al., Centre of Regenerative Medicine, Wuhan University [7]
Bone regeneration with DPSCs typically involves three components: the stem cells themselves, biocompatible scaffolds, and signalling molecules like BMP-2 or platelet-rich plasma. Together, these elements help form a mineralised bone matrix [15][10]. DPSCs also secrete bioactive substances – such as extracellular vesicles and growth factors – that encourage blood vessel formation (angiogenesis) and regulate immune responses, both of which are vital for bone healing [7][1].
A 2013 study by Giuliani and colleagues demonstrated the long-term potential of DPSCs for bone repair. Using a combination of human DPSCs and collagen sponges, they successfully treated mandibular bone defects in seven patients, with positive results observed over three years [15]. Unlike bone marrow stem cells, which require painful extraction procedures, DPSCs can be harvested from discarded wisdom teeth, making them a more convenient and less invasive option [7].
Periodontal and Soft Tissue Regeneration
DPSCs don’t stop at hard tissue repair – they also shine in regenerating soft tissues, including periodontal structures, nerves, and blood vessels. Their ability to modulate the immune response helps create a healing-friendly environment by reducing pro-inflammatory cytokines and increasing anti-inflammatory factors [10][1].
These stem cells are also highly angiogenic, meaning they can promote the formation of blood vessels. By secreting regulators like VEGF and PDGF, DPSCs stabilise blood vessels and form the microvascular networks essential for tissue health [1][9]. Additionally, research shows that DPSCs can differentiate into Schwann-like cells, which play a crucial role in regenerating peripheral nerves within soft tissues [15].
"DPSCs possess a strong angiogenic capacity to generate capillary-like structures by secreting angiogenesis regulators under certain environmental conditions."
– Kyu Hwan Kwack & Hyeon-Woo Lee, Frontiers in Cell and Developmental Biology [1]
Recent advancements include the use of 3D injectable scaffolds, such as atelocollagen and chitosan hydrogels. These scaffolds adapt to complex anatomical structures, supporting cell survival and integration [8][9]. There’s also growing interest in cell-free therapies, which rely on DPSC-derived extracellular vesicles and secretomes instead of whole-cell transplantation. These methods could simplify regulatory processes and reduce risks associated with cell-based treatments [7].
DPSCs are proving to be a versatile tool, offering new possibilities for both hard and soft tissue regeneration in dentistry. Their applications continue to expand, paving the way for more patient-friendly and effective treatments.
sbb-itb-2be92ed
Challenges and Ethical Considerations
Dental pulp stem cells (DPSCs) hold exciting potential, but moving from research labs to everyday dental clinics is no small feat. Understanding the obstacles involved helps paint a clearer picture of when these therapies might realistically become available.
Technical Challenges
Collecting DPSCs is a race against time. Once a tooth is extracted, it needs to be stored at 4°C in solutions like phosphate-buffered saline or HypoThermalsol and processed within 24 hours. Waiting longer than 10 hours significantly reduces the viability of the cells [10]. This tight timeframe can be a logistical headache, especially for dental practices that lack immediate lab support.
The methods used to isolate DPSCs also present challenges. Enzymatic digestion is quick and yields more cells but results in greater variability, while the slower explant outgrowth method produces a more uniform cell population [4][10]. These differences affect the cells’ ability to form mineralised tissue, making treatment outcomes less predictable.
Even standard root canal treatments can hinder DPSC-based regeneration. Sodium hypochlorite, a commonly used disinfectant, is toxic to DPSCs, preventing them from adhering to the root canal walls. Hua-Nien Lee from the State Key Laboratory of Oral Diseases explains:
"Sodium hypochlorite is not biocompatible and will kill DPSCs, preventing their adhesion to the root canal surface."
Additionally, mechanical preparation of the canal can destroy the stem cells already present and weaken the root wall [8].
Patient factors add another layer of complexity. While DPSCs can survive cryopreservation with up to 85% viability after two years [10], their effectiveness diminishes in older patients or those with conditions like diabetes or lupus [1]. Variability between donors – and even within a single donor – further complicates the ability to predict outcomes [4].
These technical issues are compounded by Australia’s strict ethical and regulatory landscape.
Ethical and Regulatory Aspects
Beyond the technical barriers, ethical and regulatory considerations play a crucial role in shaping how DPSC therapies progress. In Australia, the Therapeutic Goods Administration (TGA) tightly governs human cell and tissue products, including those involving DPSCs. Currently, these therapies remain in the research phase, and TGA-approved products are still "some time away" [17].
The rules are stringent but clear. Autologous stem cell treatments can bypass TGA oversight only if they are collected, processed, and administered in a hospital by a registered practitioner for a patient under their direct care [17][18]. Outside of this exemption, stem cell products must either be listed on the Australian Register of Therapeutic Goods (ARTG), used in registered clinical trials, or accessed through the Special Access Scheme for critically ill patients [16].
Direct advertising of stem cell treatments to consumers is prohibited. The TGA has expressed concerns about unproven and potentially unsafe practices:
"The TGA is concerned that some practitioners may be offering treatments that are unproven, illegal and potentially harmful."
Practitioners are also legally obligated to report adverse outcomes – such as tumours, infections, or abnormal bone growth – to help build a safety profile for these emerging therapies [16]. These regulations ensure that DPSC treatments meet rigorous safety and efficacy standards before becoming widely available.
| Regulatory Pathway | TGA Oversight Level | Key Requirements |
|---|---|---|
| TGA Approved | Full | Must be listed on the ARTG; proven safety and efficacy required |
| Hospital Use | Excluded | Limited to hospital settings; no advertising; supervised by the treating dentist |
| Clinical Trials | High | Requires informed consent, GMP-compliant manufacturing, and is typically free for patients |
| Supply Outside Hospitals | High | Rarely allowed; must involve "minimal manipulation" and comply with TGA exemptions |
Evidence-Based Care
While research into DPSCs is advancing, bringing these discoveries into routine dental care requires thorough evidence-based evaluation. In Australia, the only stem cell therapy currently approved for widespread use is haematopoietic stem cell transplantation for blood and immune disorders [17]. The TGA has stated:
"Where specific therapeutic claims are made about a product or therapy then these are supported and the product is safe."
For DPSCs to meet these standards, they must adhere to criteria set by the International Society of Cellular Therapy. This includes being plastic-adherent, expressing specific markers (CD105, CD73, CD90 ≥95%), and lacking haematopoietic markers (CD45, CD34, CD14 ≤2%) [10][12]. These benchmarks ensure consistency across studies and potential treatments.
The TGA also warns patients about the dangers of unregulated therapies:
"Undergoing an unproven stem cell treatment may interfere with proven and potentially beneficial therapies… It can also disqualify you from participation in a registered clinical trial."
This highlights the importance of pursuing DPSC treatments only through approved channels, whether via TGA-approved products, registered clinical trials, or specific hospital-based pathways [16]. While the progress in DPSC research is promising, both patients and practitioners must carefully navigate the balance between optimism and the current regulatory and scientific realities.
Future Directions in Regenerative Dentistry
Regenerative dentistry is evolving rapidly, with emerging technologies and clinical frameworks bringing dental pulp stem cell (DPSC) therapies closer to real-world application. These developments are laying the groundwork for translating these therapies into everyday clinical practice.
Advancements in Biomaterials and Techniques
One of the most exciting advancements is 3D bioprinting, which enables the precise placement of DPSCs and growth factors within custom-designed structures. This method can replicate the intricate architecture of natural dental tissues, including blood vessels and nerve pathways, offering new possibilities for dental tissue regeneration [19].
Another area gaining attention is the shift towards non-cell-based strategies, such as DPSC-derived exosomes. These tiny vesicles carry regenerative signals and offer several advantages over cell transplantation, including reduced immunogenic risks and simplified storage. As Ye Liu and colleagues noted in Frontiers in Medicine:
"Dental pulp stem cells (DPSCs) have garnered significant attention owing to their ready accessibility and minimal collection-associated risks" [7].
Additionally, cell homing is emerging as a promising technique. This approach uses bioactive molecules like granulocyte colony-stimulating factor (G-CSF) or stromal cell-derived factor 1 (SDF-1) to recruit the patient’s own stem cells to the site of injury, eliminating the need for laboratory cell expansion [8]. Another innovative method involves conditioning the root canal with EDTA, which releases growth factors embedded in the dentine to support stem cell attachment and differentiation [19].
These advancements are already showing potential in clinical settings. For instance, a 2018 randomised controlled trial led by Kun Xuan at the Fourth Military Medical University treated 40 paediatric patients with traumatised necrotic permanent incisors. The regenerated tissue not only supported continued root development but also increased dentine thickness and reduced apical foramen width – outcomes that traditional apexification techniques cannot achieve [8].
Clinical Translation of DPSC Therapies
For DPSC therapies to become part of routine clinical practice in Australia, they must meet strict regulatory standards. All cell expansion must occur in Good Manufacturing Practice (GMP)-compliant facilities to ensure safety and consistency [9]. The use of xeno-free and serum-free culture media is also critical to avoid cross-species contamination risks [20].
DPSCs’ low immunogenicity makes them well-suited for allogeneic, "off-the-shelf" transplantation. This opens the door to developing cell banks that could provide immediate treatment access [2][21].
A 2017 pilot clinical trial led by Misako Nakashima demonstrated the potential of these therapies. In this trial, autologous DPSCs mobilised from patients with irreversible pulpitis were transplanted using an atelocollagen scaffold supplemented with G-CSF. At the 24-week follow-up, three out of five patients experienced complete pulp-like tissue regeneration, with new dentine formation. Four patients also regained sensation, as confirmed through electric pulp testing [8].
However, for DPSC therapies to achieve widespread adoption in Australia, long-term studies on outcomes and cost-effectiveness are essential. These efforts will help integrate these therapies into the healthcare system and complement existing treatments.
How DPSC Therapies May Complement Existing Treatments
DPSC therapies have the potential to significantly enhance traditional dental care. For example, while conventional root canal therapy boasts a success rate of 78% to 98%, it leaves the tooth non-vital and more prone to fractures [8]. In contrast, DPSC-based regeneration aims to restore the tooth’s natural defences and sensation – functions lost during standard root canal treatments.
For immature permanent teeth, DPSC transplantation can support continued root development (apexogenesis) and apical closure, addressing the fragility often associated with traditional apexification methods [8]. As Hua-Nien Lee and colleagues from West China Hospital of Stomatology explain:
"The goal of pulp regeneration in young permanent teeth is to eliminate clinical symptoms, heal periapical lesions, regain pulp vitality, and strengthen the root canal wall" [8].
Beyond pulp regeneration, DPSCs also hold promise in implant dentistry and bone grafting. Their superior osteogenic potential makes them an excellent option for augmenting resorbed alveolar ridges. For instance, 3D-printed scaffolds seeded with DPSCs could improve outcomes in cases where conventional bone grafts have limited success [7].
With approximately 22 million root canal treatments performed annually in the United States alone – costing between $20 billion and $34 billion – the potential impact of DPSC therapies is immense [8].
| Approach | Key Advantage | Primary Application |
|---|---|---|
| 3D Bioprinting | Precise spatial control of cells/vessels | Complex tissue reconstruction |
| Cell Homing | No need for lab-expanded cells | Recruiting endogenous stem cells |
| Exosome Therapy | Low immunogenicity, easier storage | Cell-free regeneration |
| Layered Scaffolds | Mimics natural tissue interfaces | Periodontal and pulp regeneration |
Conclusion
Dental pulp stem cells (DPSCs) are opening new doors in tooth preservation and regeneration. Unlike traditional root canal therapy, which often leaves teeth lifeless and more prone to fractures, treatments using DPSCs aim to restore vital functions like blood flow, sensation, and natural defences – things conventional methods simply can’t achieve [8].
Research is already showing promising results. In 2017, Nakashima’s study highlighted nerve function restoration in most patients, while Xuan’s 2018 trial demonstrated full pulp regeneration in children, complete with functional blood vessels and continued root development – outcomes unattainable with traditional apexification [8].
That said, there are still hurdles to overcome before these therapies become routine in Australia. Challenges include the lack of standardised protocols for isolating DPSCs, the need for GMP-compliant manufacturing facilities, and the toxicity of commonly used disinfectants [8][22]. Additionally, the natural variability in DPSC quality and their reduced regenerative potential with age demand further exploration [10]. These issues highlight the critical need for more research to pave the way for clinical use.
The economic implications of current dental treatments also make it essential to conduct extensive, long-term clinical trials. These trials would need to confirm the safety, effectiveness, and cost-efficiency of DPSC-based therapies within Australia’s healthcare system.
In the meantime, dentists can take a proactive role by encouraging patients to preserve DPSCs from extracted wisdom or baby teeth. Doing so could safeguard these valuable cells for future therapeutic applications. This small step could link today’s practices with tomorrow’s regenerative solutions, as DPSC therapies have the potential to complement existing treatments and transform the future of dentistry.
FAQs
What makes dental pulp stem cells unique compared to other dental stem cells in regenerative dentistry?
Dental pulp stem cells (DPSCs) play a key role in regenerative dentistry, thanks to their ability to repair and regenerate tissues. These cells are easily sourced from adult teeth and stand out for their rapid growth, capacity to transform into various cell types (such as odontogenic, osteogenic, and neurogenic cells), and immune-modulating abilities – qualities they retain even after being cryopreserved.
When comparing DPSCs to stem cells from exfoliated deciduous teeth (SHED), DPSCs are slightly less efficient in terms of growth. However, they are more readily available in adults. SHED, on the other hand, grow faster and are particularly effective for regenerating neural tissues due to their neurogenic tendencies. Other types of dental stem cells also have their own specialised uses. For instance, stem cells from the apical papilla (SCAP) are ideal for root development and forming dentin-like tissue, while periodontal ligament stem cells (PDLSCs) excel at repairing periodontal ligaments and bone structures.
In summary, DPSCs are a great option for restoring dental pulp vitality, while SHED and other dental stem cells are better suited for focused applications, such as neural repair or root structure regeneration.
What challenges need to be overcome before dental pulp stem cell therapies can be used in everyday dentistry?
Dental pulp stem cell (DPSC) therapies have immense potential, but several obstacles must be addressed before they can become a regular part of dental care. On the biological front, the pulp space is both narrow and poorly vascularised, making it tricky to achieve consistent tissue regeneration. A major safety concern is ensuring DPSCs differentiate properly, as the formation of unintended tissue could pose risks.
From a technical perspective, challenges include establishing reliable methods to isolate and preserve DPSCs and designing biocompatible scaffolds that can effectively support cell integration. Producing GMP-grade cell products adds another layer of complexity, as this process is expensive and demands specialised facilities – resources that many dental clinics currently lack.
There are also regulatory and practical hurdles to consider. Long-term clinical data is still in its infancy, and dentists would require additional training to perform these advanced treatments. Moreover, reimbursement models for such therapies are not yet in place in Australia, making their adoption even more challenging. Overcoming these issues is a critical step toward making DPSC therapies a standard option in dental care.
How can dental pulp stem cell therapies enhance root canal treatments?
Dental pulp stem cell (DPSC) therapies are being investigated as a potential advancement in traditional root canal treatments. After the infected pulp is removed and the canal thoroughly cleaned, DPSCs – renowned for their tissue-regenerating abilities – can be introduced into the tooth using a biocompatible scaffold. These cells may help generate dentine-like tissue, blood vessels, and structures that support nerves. This could restore the tooth’s vitality and make it less prone to brittleness.
Although still in the experimental phase, early research has shown encouraging outcomes. The goal of DPSC-based therapies is to enhance standard root canal procedures by encouraging biological healing rather than simply filling the space with inert material. However, before this approach can be adopted in Australia, further research and regulatory approval will be required.
Related Blog Posts
- Mesenchymal Stem Cells in Periodontal Regeneration
- Stem Cells in Periodontal Regeneration: Current Trials
- Growth Factors vs. Stem Cells in Gum Grafting
- Recent Advances in Biomaterials for Periodontal Regeneration
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





