







Research: Systemic Diseases Mimicking Periodontitis

Did you know? Gum disease symptoms like bleeding, inflammation, and bone loss aren’t always caused by dental plaque. Systemic diseases such as diabetes, immune disorders, and genetic conditions can mimic periodontitis, making diagnosis tricky.
Here’s the key takeaway:
- Systemic diseases can cause gum damage through non-plaque-related mechanisms.
- Symptoms like rapid bone loss, unexplained inflammation, or bleeding may point to conditions like leukaemia, diabetes, or autoimmune disorders.
- Standard gum treatments often fail when systemic conditions are the real cause.
Australian dentists must recognise these warning signs, take thorough medical histories, and collaborate with doctors for accurate diagnosis and treatment. This approach not only improves oral health but can also uncover serious underlying conditions early.
BSP WEBINAR – Non-plaque induced Periodontal diseases by Prof. Iain Chapple
Systemic Diseases That Mimic Periodontitis
Certain systemic conditions can cause gum inflammation and bone loss that closely resemble plaque-induced periodontitis. However, these issues stem from entirely different systemic processes. Identifying these conditions is essential because standard periodontal treatments may not address the root cause, and oral symptoms could be the first sign of a more serious health issue requiring medical attention. Below are some key systemic conditions that can mimic periodontitis.
Diabetes Mellitus
Uncontrolled diabetes often presents symptoms similar to periodontitis. High blood sugar levels can lead to rapid loss of periodontal attachment and bone destruction. This happens due to the build-up of advanced glycation end-products (AGEs) and disruptions in inflammatory pathways, which increase levels of IL-1β, TNF-α, and IL-6 [2]. Interestingly, periodontal treatment can help lower HbA1c levels by 0.3–0.4% (3–4 mmol/mol) within three to four months [2], highlighting the close link between diabetes and periodontal health. Rather than being a separate diagnosis, diabetes acts as a modifier that exacerbates periodontitis [6][7].
Blood and Immune System Disorders
Certain blood and immune disorders, such as neutropenia, leukaemia, and HIV, can cause severe periodontal damage that doesn’t align with typical plaque-induced disease. These conditions often lead to unusual ulceration and inflammation that far outweigh the amount of dental plaque present [5]. Standard treatments like scaling and root planing often fail to resolve these cases.
- Neutropenia, characterised by a low count of neutrophils, leaves gums highly susceptible to rapid and unresolved tissue destruction.
- Leukaemia may cause gingival enlargement and spontaneous bleeding, which can serve as early warning signs of malignancy [5].
- Such symptoms should prompt immediate medical referral for further investigation and treatment.
Genetic and Autoimmune Conditions
Rare genetic disorders like Papillon–Lefèvre syndrome and Leukocyte Adhesion Deficiency (LAD) can dramatically accelerate periodontal destruction. These conditions often cause severe bone loss at a young age, leading to premature tooth loss, regardless of oral hygiene efforts. The underlying issue lies in genetic mutations that impair immune responses, making the gums highly vulnerable to damage [6][7].
Autoimmune diseases, including rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE), also affect periodontal health in unique ways. A study in Nature notes, "Periodontitis and RA exhibit several common features, including shared pathogenetic processes, cytokine profiles, inflammatory markers and genetic associations" [2]. The oral bacterium Porphyromonas gingivalis plays a role here by producing citrullinated proteins, which are linked to RA. Additionally, individuals with Down syndrome often face severe periodontal issues due to immune system dysfunction [6].
How Systemic Diseases Cause Periodontitis‑Like Symptoms
Understanding the biological connections between systemic diseases and periodontal-like symptoms sheds light on why standard treatments for periodontitis sometimes don’t work. These conditions often involve additional inflammatory processes that contribute to tissue damage.
Shared Inflammatory Pathways
Systemic inflammation can ramp up levels of IL‑1, IL‑6, and TNF‑α, which circulate throughout the body and worsen periodontal tissue damage [8][2]. Some individuals have an overactive immune response, where Toll‑like receptor activation leads to excessive inflammatory mediator production. This not only heightens the severity of periodontitis but also increases the risk of systemic issues like endothelial dysfunction [2]. Another key factor is the RANK‑L pathway, which promotes osteoclast activity. This process drives bone loss, a hallmark of periodontitis, and is also seen in conditions like diabetes and osteoporosis [8][2]. Additionally, matrix metalloproteinases (MMPs), activated by inflammatory cytokines, contribute to the breakdown of connective tissues [8][2].
"Chronic periodontitis therefore represents a source of chronic inflammation that may be a significant contributing factor in the pathogenesis of other inflammatory based diseases."
– Lewis Winning and Gerard J. Linden, Queen’s University Belfast [1]
Elevated C‑reactive protein (CRP) levels, typically between 3 mg/L and 10 mg/L, are often linked to periodontitis. This low-grade inflammation might not show obvious symptoms but can lead to secondary complications [8]. These inflammatory processes also influence the balance of bacteria in the mouth.
Changes to Oral Bacteria and Systemic Effects
Systemic diseases can disrupt the oral environment, creating conditions that favour harmful bacteria. For instance, in diabetes, elevated glucose levels in the gums encourage the growth of disease-causing bacteria, altering the oral microbiome [8][2].
Chronic inflammation in the body can increase IL‑17 expression in oral tissues, which supports the growth of pathogenic bacterial communities [8]. Immune-compromising conditions like neutropenia or Leukocyte Adhesion Deficiency further disrupt the regulation of oral microbes, leading to an imbalance known as dysbiosis [4][8]. With the oral microbiota including 500 to 700 common bacterial species, even minor disturbances can have a big impact [8].
Systemic oxidative stress and inflammation can weaken the integrity of epithelial barrier proteins like claudins and E‑cadherins. This increases gingival permeability, allowing oral bacteria to enter the bloodstream [8]. Interestingly, periodontal therapy has been shown to lower the risk of hospital-acquired pneumonia by about 40% [2]. Such findings highlight why standard periodontal treatments might fall short when systemic conditions are at play.
Blood Vessel and Metabolic Changes
Beyond inflammation and bacterial shifts, vascular and metabolic changes further worsen periodontal damage. Endothelial dysfunction, a warning sign of vascular disease, can happen when periodontal bacteria like Porphyromonas gingivalis enter the bloodstream, triggering inflammation in the blood vessel walls [1][2]. Pro‑inflammatory cytokines also increase vascular permeability, which allows immune cells to infiltrate and form chronic inflammatory lesions – even when plaque is minimal.
In diabetes, advanced glycation endproducts (AGEs) bind to their receptors (RAGE) in the periodontium, increasing oxidative stress and tissue destruction through higher reactive oxygen species (ROS) levels [2][8]. Similarly, metabolic syndrome and high-fat diets elevate RANKL levels, which promote bone loss by enhancing osteoclast activity.
Microangiopathy, or damage to small blood vessels, reduces the delivery of oxygen and nutrients to periodontal tissues. This impairs healing and mimics the tissue damage seen in periodontitis. These interconnected pathways emphasise the importance of managing systemic diseases to improve periodontal health.
| Mechanism | Biological Impact on Periodontium | Associated Systemic Condition |
|---|---|---|
| AGE/RAGE Interaction | Increased oxidative stress and heightened inflammation | Diabetes Mellitus |
| Endothelial Dysfunction | Reduced vascular function and elevated adhesion molecules | Cardiovascular Disease |
| MMP Activation | Breakdown of connective tissue and bone matrix | Metabolic Syndrome / Obesity |
| RANKL Elevation | Enhanced bone resorption and alveolar bone loss | Obesity / High‑fat diets |
| Vascular Permeability | Chronic inflammation due to immune cell infiltration | Chronic Systemic Inflammation |
sbb-itb-2be92ed
Diagnosing Systemic Diseases That Mimic Periodontitis
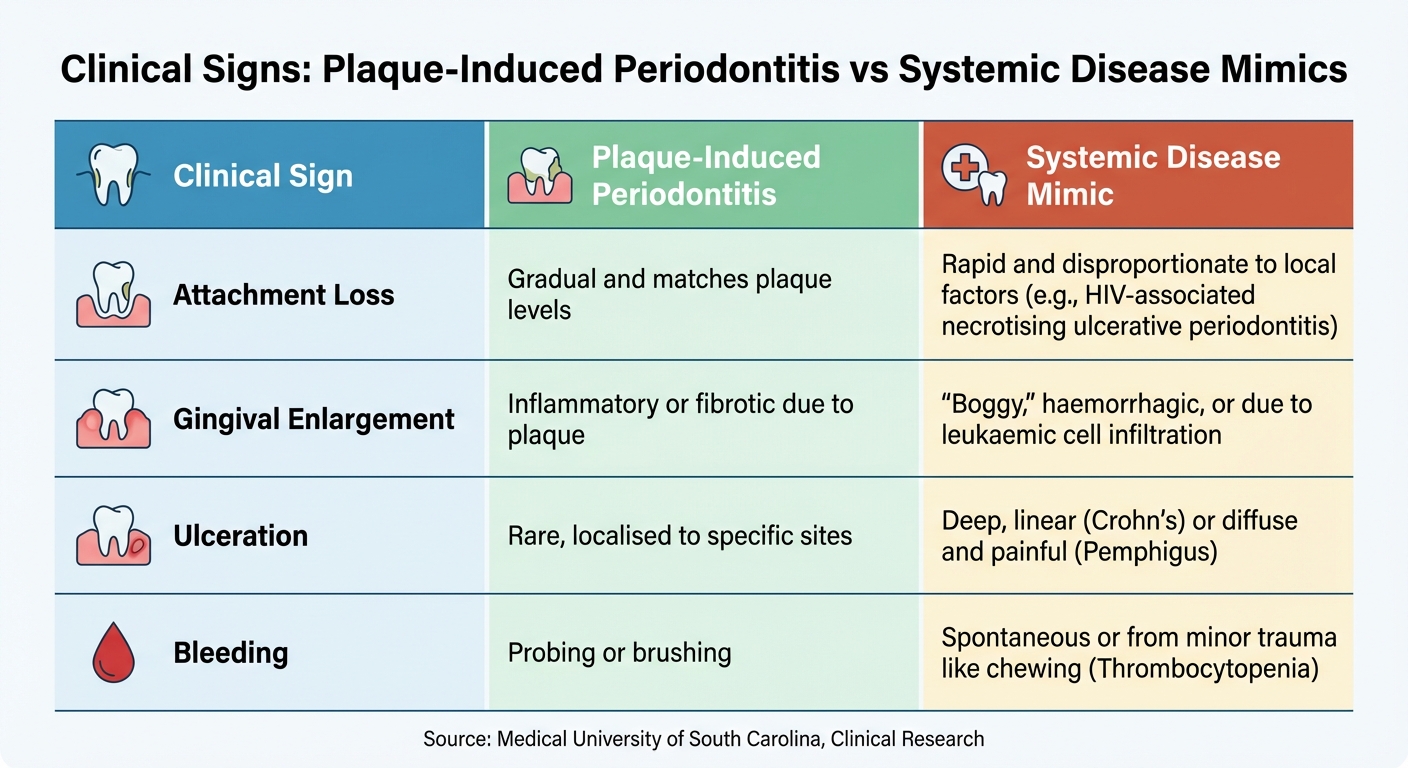
Clinical Signs: Plaque-Induced Periodontitis vs Systemic Disease Mimics
Identifying systemic diseases that resemble periodontitis calls for a thorough and structured approach. When standard periodontal treatments fail to resolve inflammation despite good plaque control, it’s essential to consider underlying systemic conditions. Australian dental professionals should be alert to specific warning signs, take detailed medical histories, and collaborate with medical practitioners when necessary.
Clinical Warning Signs of Systemic Disease
Certain clinical signs should raise suspicion of systemic conditions masquerading as periodontal disease. One key indicator is rapid attachment loss that doesn’t align with the level of dental plaque. For instance, significant bone loss with minimal plaque or persistent gingival inflammation despite proper therapy and plaque control may point to an underlying systemic issue[5][9][11]. Similarly, severe periodontal destruction in children or young adults could signal rare genetic disorders like Papillon-Lefèvre Syndrome, leukocyte adhesion deficiency, or hypophosphatasia[10].
Distinctive gingival changes can also provide clues. Features like "cobblestone" mucosa, deep linear ulcerations, or persistent firm swelling of the lips and cheeks may indicate Crohn’s disease[9]. Spontaneous gingival bleeding or bleeding from minor trauma, such as chewing, could suggest conditions like thrombocytopenia or leukaemia rather than plaque-induced inflammation[9]. Additionally, systemic symptoms such as skin lesions, joint pain, or unexplained weight loss should heighten clinical suspicion[9][10].
These signs highlight the importance of a detailed medical history and further investigation.
| Clinical Sign | Plaque-Induced Periodontitis | Systemic Disease Mimic |
|---|---|---|
| Attachment Loss | Gradual and matches plaque levels | Rapid and disproportionate to local factors (e.g., HIV-associated necrotising ulcerative periodontitis)[9] |
| Gingival Enlargement | Inflammatory or fibrotic due to plaque | "Boggy", haemorrhagic, or due to leukaemic cell infiltration[9] |
| Ulceration | Rare, localised to specific sites | Deep, linear (Crohn’s) or diffuse and painful (Pemphigus)[9] |
| Bleeding | Probing or brushing | Spontaneous or from minor trauma like chewing (Thrombocytopenia)[9] |
Medical History and Clinical Examination
Once potential red flags are identified, a detailed medical history and clinical examination are critical. Begin by evaluating smoking habits, as smoking – classified as a chronic relapsing disorder (ICD-10 F17) – increases the risk of periodontitis by 2- to 5-fold[10]. Screening for diabetes is also essential, as poorly controlled hyperglycaemia accelerates periodontal attachment loss significantly[9].
During the exam, assess the periodontal phenotype using a probe to measure gingival thickness. If the probe is visible through the tissue, the phenotype is considered thin (≤1 mm), which increases the risk of gingival recession and rapid attachment loss[10]. Historical indicators like skin lesions, abdominal pain, or unusual medication use can further suggest systemic involvement[5][11].
Oral lesions often serve as early warning signs of systemic diseases. For example, in 50% to 80% of pemphigus vulgaris cases, oral lesions appear before skin symptoms – sometimes by over a year[9]. Chronic oral ulceration warrants testing for the Nikolsky sign, where firm lateral pressure on normal-appearing mucosa can cause blistering, a hallmark of pemphigus vulgaris[9]. Other atypical presentations, such as linear gingival erythema or necrotising ulcerative periodontitis with rapid attachment loss and spontaneous bleeding, may strongly indicate underlying HIV infection[9].
"Oral lesions often are the first manifestation of disease and may precede the onset of skin lesions."
– Angela C. Chi, DMD, Associate Professor, Medical University of South Carolina[9]
Laboratory Tests and Medical Referrals
When systemic disease is suspected, confirming the diagnosis through laboratory tests and medical referrals is vital. For conditions like leukaemia, neutropenia, or unexplained gingival bleeding, a complete blood count (CBC) and platelet count can help identify blood disorders[9][10]. Thrombocytopenia, for instance, may first manifest as oral lesions when platelet counts drop below 50 × 10³ per μL[9].
If diabetes is suspected or confirmed, ordering an HbA1c test and coordinating care with the patient’s GP or diabetes specialist ensures effective management[9][12]. Localised gingival enlargements that appear "boggy" or haemorrhagic should prompt immediate referral for potential leukaemic infiltration or neoplastic disease[9][10]. For non-plaque-induced lesions, such as oral squamous cell carcinoma or immune-mediated conditions like pemphigus vulgaris, a biopsy is often necessary for a definitive diagnosis[9][11].
Collaboration between dental practitioners, general practitioners, and medical specialists is essential for early detection and treatment of systemic conditions. For example, in Australian dental settings, diffuse melanin pigmentation in the oral mucosa may require a broad differential diagnosis, including Addison’s disease, ethnic pigmentation, or medication-related changes[9].
Managing Patients with Systemic Disease Mimics
Once a correct diagnosis is made, managing systemic conditions that resemble periodontitis becomes crucial for maintaining both oral and overall health. Recognising these mimics calls for a coordinated effort between medical and dental care to address the root causes while reducing oral inflammation. For Australian dental practitioners, it’s important to view factors like diabetes and smoking as modifying elements within the diagnosis rather than treating them as separate conditions [7]. This collaborative approach paves the way for better treatment outcomes and long-term health improvements.
Treatment Outcomes and Prognosis
Early detection and proper medical management of systemic conditions can lead to noticeable improvements in periodontal health and general well-being. Non-surgical periodontal treatments, such as professional plaque removal and oral hygiene education, have shown to enhance glycaemic control in diabetic patients. Studies indicate reductions in HbA1c levels by 0.5%–1.5% within three months [14], along with a potential decrease in cardiovascular risks. These benefits often extend for at least a year [12].
"For patients with diabetes and periodontitis, provide periodontal treatment, including oral hygiene instruction and supra- and subgingival professional mechanical plaque removal (PMPR), with the aim of reducing oral inflammation and improving diabetes control." – Scottish Dental Clinical Effectiveness Programme (SDCEP) [12]
Research also links periodontal therapy to a 10–14% decrease in major cardiovascular events over a decade [14]. For pregnant women with periodontitis – who face higher risks of preterm birth and preeclampsia [14] – periodontal care can help reduce potential risks to the baby’s health. However, practitioners should note that poorly managed systemic conditions can impair wound healing, making traditional periodontal treatments more complicated and less predictable [12].
To maintain these positive outcomes, personalised care plans tailored to individual needs are essential.
Personalised Oral Health Care Plans
Customised treatment plans are a cornerstone of effective care for patients with systemic disease mimics. These plans should consider whether the systemic condition worsens plaque-induced inflammation (e.g., diabetes or rheumatoid arthritis), leads to immune or tissue defects (such as Down syndrome or Papillon-Lefèvre syndrome), or causes tissue damage unrelated to plaque (as seen in Langerhans cell histiocytosis) [4].
Tailor oral hygiene advice and maintenance routines to the patient’s specific risks [12]. Non-surgical treatments, including professional mechanical plaque removal, aim to reduce oral inflammation and, in turn, the body’s overall inflammatory burden [12][3]. Maintenance schedules should be adjusted based on individual risk factors, using tools like mathematical algorithms that factor in age, smoking, diabetes, and radiographic bone height to predict future attachment loss [13].
For high-risk patients, such as those with leukaemia or undergoing chemotherapy, preventive measures like chlorhexidine rinses, acyclovir, or nystatin may be necessary to minimise issues like mucositis or opportunistic infections [9]. Patients with Crohn’s disease might benefit from topical or intralesional corticosteroids for stubborn oral lesions [9]. Special precautions are also needed for patients with unstable cardiovascular conditions, as full-mouth periodontal procedures could pose additional risks [12].
Considerations for Australian Dental Practice
In Australia, established guidelines and strong inter-professional communication are key to managing these complex cases effectively. Building active communication channels with general practitioners and specialists – such as diabetes care teams – ensures seamless co-management [12][14]. This two-way collaboration allows dental professionals to act as frontline identifiers of systemic issues by recognising oral signs that require further medical evaluation [5].
"Inter-professional collaboration and partnership are advocated for the co-management of medical and dental conditions that are linked, but currently managed by separate groups of healthcare professionals." – Annals Academy of Medicine Singapore [14]
Incorporating systemic factors like diabetes and smoking into periodontitis diagnoses is essential [7][6]. Standardised referral templates that highlight critical oral signs – such as rapid attachment loss or unresponsive gingival lesions – help strengthen integrated care [14][5]. For patients with neurodegenerative disorders like Alzheimer’s or Parkinson’s, who may struggle with manual dexterity, working closely with medical teams and caregivers to create tailored oral hygiene strategies is vital [2].
With severe periodontitis affecting around 1.1 billion people globally and ranking as the sixth most common health condition [14], Australian dental practitioners have a significant role in reducing morbidity and mortality by accurately diagnosing and managing these systemic disease mimics [5].
Conclusion
For Australian dental practitioners, identifying systemic diseases that resemble periodontitis is a critical step in ensuring accurate diagnosis and effective treatment. Some conditions, such as oral squamous cell carcinoma, can manifest with symptoms similar to periodontal disease but demand immediate medical attention rather than conventional periodontal care [10][11]. Recognising lesions unrelated to plaque early on enables timely referrals to medical specialists, which can significantly lower patient morbidity and mortality rates [5][11].
"Dental practitioners should be aware of the various manifestations of systemic diseases to the periodontium in order to offer appropriate diagnosis and treatment, which can reduce both patient morbidity and mortality." – Josefine Hirschfeld, Department of Periodontology, Birmingham Dental School [5]
The 2017 World Workshop framework provides a structured approach, differentiating conditions that modify periodontitis (like diabetes and rheumatoid arthritis) from those causing attachment loss that isn’t linked to plaque. This framework encourages moving beyond standard plaque control and tailoring care to individual patient needs [10][4][8]. By being vigilant for unusual presentations and keeping an eye on systemic factors such as smoking and glycaemic levels, dental professionals can better predict how diseases may progress [10].
Collaboration across disciplines becomes indispensable in managing these complex cases effectively. Dentists are often in a unique position to spot early warning signs of systemic conditions that might otherwise go undiagnosed. This proactive approach not only enhances oral health outcomes but can also contribute to broader health improvements, such as better glycaemic control for diabetic patients [1][8].
FAQs
How does diabetes impact gum health?
Diabetes can have a noticeable impact on gum health, primarily by weakening the immune system and slowing down the body’s ability to heal. Elevated blood sugar levels reduce the body’s ability to fight off infections, making gums more susceptible to issues like gingivitis and periodontitis. For those with poorly managed diabetes, the risk of accelerated damage to gum tissues and bone is even higher.
Interestingly, the relationship works both ways. Gum disease can make diabetes management more challenging by increasing systemic inflammation, which can lead to higher blood sugar levels. On the flip side, improving gum health – through professional dental care and consistent oral hygiene – can slightly lower blood sugar levels, offering a small but meaningful boost to diabetes control.
For individuals with diabetes, protecting gum health is crucial. This includes regular dental visits, brushing twice daily with fluoride toothpaste, flossing daily, and keeping blood sugar levels in check. Taking these steps not only supports healthy gums but also contributes to better overall health.
What signs suggest gum problems might be linked to an underlying health condition?
Gum problems linked to systemic diseases often stand apart from the more common plaque-related gum issues. Some key signs to be mindful of include persistent or excessive bleeding, noticeable and rapid gum deterioration (like pocket depths increasing over 2 mm in just weeks), and pain or ulcers that don’t improve despite regular oral care. Other indicators might involve unusual changes in the mouth, such as pale or inflamed gums, white patches, or severe inflammation in areas that were previously healthy.
Certain systemic conditions – such as diabetes, HIV, leukaemia, or autoimmune disorders – can have a significant impact on gum health. These conditions may lead to refractory periodontitis, which doesn’t respond well to standard treatments, slower healing after dental procedures, or pronounced bone loss. If these dental symptoms occur alongside broader health concerns like unexplained fatigue, weight loss, or fever, it’s crucial to seek advice from both your dentist and a medical professional to investigate potential underlying causes.
Why might periodontal treatments not work when a systemic disease is involved?
Periodontal treatments can sometimes fall short when the symptoms stem from a systemic or immune-mediated condition. Unlike gum disease triggered by plaque buildup, these conditions often involve inflammation driven by the body’s immune response or another underlying systemic issue. Standard treatments like scaling, root planing, or antimicrobial therapies might not tackle the actual cause and, in some cases, could even exacerbate the problem.
This underscores how critical it is to identify systemic diseases that resemble periodontal problems to ensure patients receive the right combination of medical and dental care.
Related Blog Posts
- 5 Early Signs of Gum Disease
- Diabetes and Periodontitis: Oral Microbiome Changes
- Periodontal Disease in Lupus Patients: Key Facts
- Differential Diagnosis for Periodontal Infections
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





