







Systemic Health and Periodontal Risk: Osteoporosis Insights

Osteoporosis weakens bones, while periodontal disease harms gums and teeth. These conditions may worsen each other through shared biological mechanisms like inflammation and hormonal changes. Key points include:
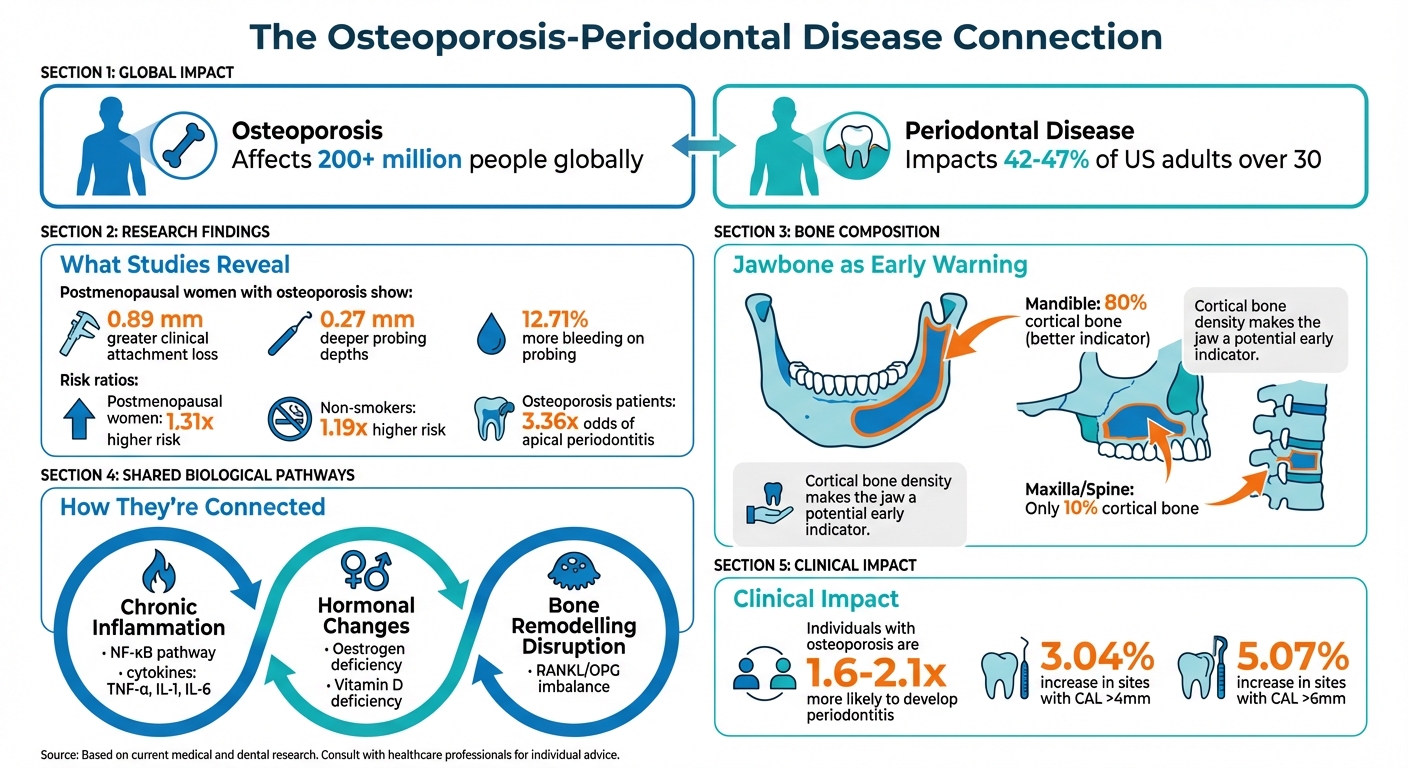
- Osteoporosis affects over 200 million people globally, increasing fracture risks.
- Periodontal disease impacts 42–47% of adults over 30 in the US, leading to gum and bone damage.
- Research shows individuals with low bone density are more prone to severe periodontal issues, such as gum attachment loss.
- Dental X-rays can reveal jawbone changes linked to osteoporosis, aiding early detection.
By linking bone and oral health care, professionals can detect risks earlier and improve patient outcomes. Collaboration between dentists and doctors is essential, especially for managing treatments like bisphosphonates, which carry risks like jawbone complications.
Quick Facts:
- Postmenopausal women with osteoporosis show worse gum health outcomes.
- Inflammation and oestrogen deficiency drive bone loss in both conditions.
- Routine dental X-rays can be a practical tool for spotting early signs of osteoporosis.
A combined approach to bone and gum health can help prevent complications and improve quality of life.
Osteoporosis and Periodontal Disease Connection: Key Statistics and Risk Factors
Research Connecting Osteoporosis and Periodontal Health
What Recent Studies Show
Research continues to shed light on the connection between low bone mineral density and periodontal health. A 2023 meta-analysis of 28 observational studies involving 19,611 patients revealed that postmenopausal women with osteoporosis had noticeably worse periodontal outcomes compared to those with normal bone density. These women experienced 0.89 mm greater clinical attachment loss, 0.27 mm deeper probing depths, and 12.71% more bleeding on probing [8].
"Postmenopausal osteoporosis patients are more likely to suffer from periodontitis, and the condition is easily aggravated." – Jing Qi et al., Lanzhou University [8]
Further studies reinforce this link, showing that individuals with low bone density tend to have more sites with severe attachment loss. A five-year cohort study involving 2,418 participants found that baseline osteoporosis increased the likelihood of periodontitis progression. Postmenopausal women in this group had an adjusted risk ratio of 1.31, while non-smokers had a ratio of 1.19 [9]. This highlights a two-way relationship: severe periodontitis may also contribute to systemic bone loss through inflammation triggered by bacteraemia [6]. These findings underscore the importance of combining periodontal health checks with bone health assessments to catch issues early. For instance, jaw bone changes could serve as a practical way to identify systemic osteoporosis before more serious complications arise.
Jaw Bone Changes as Early Warning Signs
Jaw bone structure changes, particularly in the mandible, can act as early signs of systemic osteoporosis. Routine dental X-rays can reveal these changes, making them a valuable screening tool. The mandible, which consists of up to 80% cortical bone, provides a better indication of cortical bone health than the maxilla or spine, which are only about 10% cortical bone [1]. Indicators like thinning of the Mandibular Cortical Width and changes in trabecular patterns – such as more spaced and disconnected bone – are closely linked to systemic bone mineral density loss [1][6].
This connection opens up opportunities for proactive screening. Dental professionals reviewing panoramic radiographs can spot these structural changes and recommend bone density testing, potentially preventing fractures. A large-scale study of 1,644,953 patients found that osteoporosis patients had a significantly higher prevalence of apical periodontitis, with an odds ratio of 3.36 [10]. These findings highlight the importance of collaboration between dental and medical professionals to identify at-risk patients early, paving the way for more integrated and effective care approaches.
Biological Pathways Linking Both Conditions
How Inflammation Affects Both Conditions
Chronic inflammation plays a central role in both osteoporosis and periodontal disease, driving bone loss through interconnected cellular processes. Inflammation activates the Nuclear Factor-kappa B (NF-κB) signalling pathway, which promotes the formation of osteoclasts (cells that break down bone) while suppressing osteoblast activity (cells that build bone). This happens through pro-inflammatory cytokines like TNF-α, IL-1, and IL-6, which increase RANKL levels and lower osteoprotegerin (OPG). This imbalance in the RANK/RANKL/OPG system creates conditions where bone breakdown surpasses bone formation [1][7][11].
"The cytokines activated during the course of inflammatory responses have profound effects on the differentiation and activity of osteoblasts and osteoclasts and, therefore, are considered to be mediators of inflammation-associated osteoporosis and periodontitis."
– Bo Yu, Division of Regenerative and Constitutive Sciences, UCLA [1]
A fascinating discovery in recent research is "trained osteoclastogenesis", where immune memory causes myeloid progenitors to undergo epigenetic changes, making them more likely to become osteoclasts during future inflammatory episodes [11]. On top of this, neutrophils and macrophages release matrix metalloproteinases (MMPs) and reactive oxygen species (ROS), which degrade the extracellular matrix and weaken bone structure [11][12].
While inflammation is a major driver, hormonal factors also play a key role in worsening bone loss, as explored next.
Effects of Oestrogen Deficiency and Vitamin D
Oestrogen deficiency, especially after menopause, disrupts the balance of bone remodelling. It increases pro-inflammatory cytokines and osteoclast activity while boosting RANKL expression, tipping the RANKL/OPG ratio towards bone resorption. This accelerates the loss of both skeletal and alveolar bone [2][3][6][13].
A 1999 study by Payne et al. followed 58 postmenopausal women (41 with normal bone density and 17 with osteoporosis) in a periodontal maintenance program. Women with osteoporosis and oestrogen deficiency showed significantly greater alveolar bone loss and reduced bone density in the jaw over time [1][6].
Vitamin D is equally important. It regulates parathyroid hormone (PTH) levels and helps the body absorb calcium from the gut. When vitamin D levels drop, the body compensates by pulling calcium from bones, weakening them in the process [3]. Low vitamin D levels also worsen systemic inflammation, amplifying the immune response to periodontal pathogens [3]. Research has shown that vitamin D deficiency (below 20 nmol/L) negatively impacts periodontal surgery outcomes, with effects lasting up to a year [2].
Disrupted Bone Remodelling Processes
The combined effects of chronic inflammation and hormonal deficiencies disrupt the delicate balance between bone formation and resorption – a phenomenon referred to as "uncoupling" of bone remodelling [1][3]. Under normal conditions, osteoclasts and osteoblasts work in harmony to maintain bone health. However, inflammation and hormonal changes tilt this balance, causing osteoclastic activity to outpace the bone-building efforts of osteoblasts.
Chronic periodontal inflammation further raises systemic RANKL and cytokine levels, speeding up skeletal bone loss in individuals vulnerable to osteoporosis [6]. The jawbone, especially the mandible, becomes particularly susceptible. As systemic osteoporosis reduces its mineral density, the periodontium is left more vulnerable to infections from oral biofilms.
"Osteoporosis of the alveolar bone may constitute a ‘weakened resistance’ of the periodontium to infectious challenge."
– Chin-Wei (Jeff) Wang, Department of Periodontics and Oral Medicine, University of Michigan [7]
Interestingly, emerging evidence points to the role of gut health in bone stability. Metabolites like butyrate, produced by gut bacteria, may encourage regulatory T cells that suppress osteoclast activity. This suggests a potential link between gut health, osteoporosis, and periodontal disease [3].
Applying This Knowledge in Clinical Practice
How Osteoporosis Affects Periodontal Disease Risk
Osteoporosis has a direct impact on periodontal health, increasing the need for early detection and tailored treatment plans. Changes in jawbone structure, as seen in osteoporosis, can be identified through routine panoramic radiographs. Look out for signs like reduced mandibular cortical width and disrupted trabecular patterns, which may indicate low systemic bone mineral density (BMD) [17][6].
Clinical Attachment Loss (CAL) is a key marker when evaluating periodontal risk in patients with osteoporosis. Research shows that low BMD is associated with a 3.04% rise in sites with CAL >4 mm and a 5.07% increase in sites with CAL >6 mm [1]. Additionally, menopausal and osteoporotic women are at a higher risk of moderate-to-severe periodontitis, with odds increasing by 1.66-fold and 1.25-fold, respectively [6].
A comprehensive evaluation should include systemic risk factors such as postmenopausal status, deficiencies in vitamin D and calcium, and the use of antiresorptive medications like bisphosphonates or denosumab. Prior to starting antiresorptive therapy, ensure the patient receives dental clearance to lower the risk of medication-related osteonecrosis of the jaw (MRONJ) [6]. For patients showing rapid alveolar bone loss, referring them for a DXA scan can provide further insights. These steps lay the groundwork for integrated and effective treatment strategies.
Coordinated Care Between Dental and Medical Professionals
Managing patients with both osteoporosis and periodontal disease calls for a team approach, bridging dental and medical care. Collaboration between dental surgeons and medical practitioners is essential. Mutual referrals play a critical role here: dental professionals should refer patients with severe periodontitis to rheumatologists for BMD evaluations, while medical practitioners should encourage osteoporosis patients to schedule regular dental check-ups to prevent complications like tooth loss [15][4].
"The close association between osteoporosis and periodontitis should lead dental surgeons to refer patients with severe periodontitis to a rheumatologist for an assessment of bone density."
– Françoise Tilotta, Marjolaine Gosset, Julia Herrou, Karine Briot, and Christian Roux [4]
Clear communication protocols between healthcare providers are crucial, especially when coordinating the timing of dental procedures and antiresorptive therapies [16]. Medical professionals can advise their patients that maintaining excellent oral hygiene and consistent dental care is the most effective way to minimise MRONJ risk while continuing necessary treatments [14].
Nutritional counselling should also be a part of this interdisciplinary approach. Recommendations include 1,000–1,200 mg of calcium and 600–800 IU of vitamin D daily to support systemic bone health and periodontal stability. Address modifiable risk factors such as smoking, poor diabetes control, and imbalanced nutrition to optimise outcomes for both osteoporosis and periodontal disease [17][16][6]. Dentists can further enhance care by incorporating tools like the Fracture Risk Assessment (FRAX) into routine screenings for postmenopausal patients [16][6]. This approach highlights the importance of addressing systemic bone health as part of periodontal disease management.
sbb-itb-2be92ed
What We Still Need to Learn
The Need for Better Study Designs
Despite growing interest, the connection between osteoporosis and periodontal disease remains unclear. Most research relies on cross-sectional studies, which can show associations but fall short of proving cause-and-effect relationships between systemic bone loss and periodontal destruction. This gap leaves healthcare providers without clear guidance on how these conditions might influence one another over time [6][7]. To improve collaboration between dental and medical professionals, closing these research gaps is essential.
A major barrier is the inconsistent diagnostic criteria used across studies, making comparisons and meta-analyses challenging [1][5]. For example, a systematic review revealed conflicting findings: six studies reported a positive link between osteoporosis and periodontal health measures, while five found no such connection [7]. This inconsistency underscores the need for standardised measurement protocols to produce more reliable data.
"The association between osteoporosis and the clinical parameters of periodontitis are still inconclusive… but there is a significant association with tooth loss."
– Chin-Wei (Jeff) Wang, Department of Periodontics and Oral Medicine, University of Michigan [7]
Another limitation is the narrow focus of study cohorts. Most research centres on postmenopausal women, leaving significant gaps in data for men, premenopausal women, and individuals from various ethnic backgrounds [1][6]. Additionally, factors like smoking, ageing, and diabetes are often not fully accounted for, making it difficult to pinpoint the direct impact of osteoporosis on periodontal health [3][6].
These shortcomings highlight the urgent need for research that not only addresses these gaps but also explores new prevention strategies.
Developing Better Prevention Strategies
To determine whether treatments for osteoporosis can also improve periodontal health, longitudinal studies are crucial. These studies could provide insights into whether antiresorptive medications lead to measurable improvements in periodontal attachment levels. As Naif Alwithanani from Taif University explains, "Future research should prioritise longitudinal studies, biomarker development, and integrated care models to advance the precise management of these interconnected diseases" [6].
Developing advanced tools for early detection and prevention is also a priority. Researchers are exploring biomarker panels from saliva, serum, and gingival crevicular fluid to create dual-risk prediction tools for skeletal and oral bone loss [3][6]. Additionally, cutting-edge imaging technologies like high-resolution peripheral quantitative CT (HR-pQCT) could help map jawbone microarchitecture in patients receiving osteoporosis treatments [6].
There’s growing interest in the "gut-bone-periodontal axis" – an area investigating how gut microbiota metabolites might influence both systemic and oral bone health [3]. This emerging field could pave the way for prevention strategies that address shared risk factors, offering a more integrated approach to managing these interconnected conditions.
Osteoporosis and Dental concerns | OsteoDental Link Unveiled | Oral health and chronic condition
Conclusion
Research clearly shows a strong link between osteoporosis and periodontal disease. These conditions are connected through shared biological mechanisms, such as the RANKL/OPG pathway and chronic inflammation, creating a cycle where systemic bone loss and alveolar bone loss exacerbate one another. Studies reveal that individuals with osteoporosis are 1.6 to 2.1 times more likely to develop periodontitis than those with normal bone mineral density (BMD). Considering that osteoporosis affects over 200 million people globally and periodontitis impacts about 42% of American adults aged 30 or older [1], this relationship has serious public health consequences. It highlights the need for a combined clinical approach.
The solution lies in collaboration between dental and medical professionals. Chin-Wei (Jeff) Wang from the University of Michigan emphasises this point:
"Defining the relationship between osteoporosis and periodontitis will help identify patients with one disorder who are at a higher risk for developing the other, and thereby could benefit from coordinated interdisciplinary care" [7].
Practical steps, such as dentists identifying mandibular cortical thinning on routine X-rays or doctors referring osteoporosis patients for periodontal assessments, can lead to earlier detection of both conditions. This type of teamwork ensures timely interventions and more thorough treatment plans, leading to better patient outcomes.
Evidence also suggests that integrated care can lower systemic inflammation while preserving alveolar bone [6]. However, this approach requires careful planning to avoid complications, such as medication-related osteonecrosis of the jaw, particularly when using treatments like bisphosphonates or denosumab [3][6].
Although further research is needed, the current findings strongly support a unified strategy. For patients dealing with either condition, understanding this connection offers an opportunity for more holistic care that addresses both bone and oral health. These insights lay the groundwork for better outcomes through effective, interdisciplinary collaboration.
FAQs
How does osteoporosis affect oral health?
Osteoporosis can weaken the jawbone, which is crucial for supporting your teeth and preserving the overall structure of your mouth. When bone density decreases, it can lead to jawbone loss, increasing the likelihood of loose teeth or even tooth loss.
This condition shares several risk factors with periodontal disease, including age, smoking, and hormonal changes – the latter being particularly common in postmenopausal women. Chronic gum inflammation caused by periodontal disease can also accelerate bone loss, creating a stronger connection between the two issues. Because of this, prioritising good oral hygiene and scheduling regular dental check-ups becomes especially important if you have osteoporosis or are at risk of developing it.
How can dental X-rays help in identifying osteoporosis?
Dental X-rays, particularly panoramic radiographs, play a role in spotting early signs of osteoporosis. By examining the thickness of the mandibular cortex and noting changes in bone density, these images can reveal potential reductions in bone strength and an increased fracture risk.
Such observations can lead to timely referrals for additional medical tests, aiding in early diagnosis of osteoporosis and possibly improving health outcomes.
Why is it important for dentists and doctors to work together when managing osteoporosis and periodontal disease?
When it comes to managing osteoporosis and periodontal disease, teamwork between dentists and doctors plays a crucial role. These two conditions are closely linked, sharing common risk factors and affecting bone health in different but interconnected ways. Osteoporosis weakens bones throughout the body, while periodontal disease leads to bone loss around the teeth. Studies have shown that poor bone health can aggravate gum disease, and the reverse is also true.
By working together, dentists and doctors can provide a more comprehensive approach to care. Dentists, during routine oral health assessments, can identify signs of systemic bone loss, potentially flagging early indicators of osteoporosis. Meanwhile, doctors can consider a patient’s gum health when assessing their risk for osteoporosis. This collaboration allows for early detection and coordinated treatment, improving outcomes for both oral and overall health.
Addressing shared factors like ageing, hormonal changes, and inflammation requires input from both medical and dental professionals. By combining their expertise, they can tackle these overlapping issues more effectively, ensuring patients receive the care they need for better long-term health.
Related Blog Posts
- Diabetes and Periodontitis: Oral Microbiome Changes
- Periodontal Disease in Lupus Patients: Key Facts
- Systemic Conditions Impacting Osseointegration
- Research: Systemic Diseases Mimicking Periodontitis
Important Notice: Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.
Individual results may vary. The information provided in this article is for educational purposes only and does not constitute medical advice.
Checkout Related Blogs




Get in touch with us
For more information, call us now to start feeling better. Or fill the form below to make appointment
The Latest News from Complete Smiles
How to Clean Clear Plastic Retainers
Checklist for Choosing Wearable Dental Devices
Checklist for Choosing Cloud AI Platforms in Dentistry

Complete Smiles Bella VistaAccepts All Major Health Funds, Including





